Salmonella typhi infection causing prolonged chronic illness and cutaneous leucocytoclastic vasculitis in a patient with IL-12 receptor β1 deficiency
Abstract
Background: Interleukin-12 Receptor β1 (IL-12Rβ1) deficiency causes susceptibility to weakly virulent atypical mycobacteria and Salmonella. Genotype–phenotype correlations are weak and penetrance is not complete. Most of the culture-recovered Salmonella are with the non typhi types.
Case report: We describe an 11 year old male patient with IL-12Rβ1 deficiency. He had an erythematous rash resembling Henoch Schonlein Purpura, and initially presented with slightly elevated CRP. Skin biopsy revealed leukocytoclastic vasculitis. Due to lack of evidence of an active infection, positive ANA, and positive direct Coombs test, an autoimmune lupus-like disease was suspected. In conjunction with rash flares, he showed progressively elevated inflammatory markers, chronic anemia, and hypoalbuminemia. Extensive investigations for an infectious etiology were negative, and without isolation of any pathogens. However, the last of a series of abdominal ultrasound examinations revealed enlarged peritoneal and retroperitoneal lymph-nodes, and biopsy yielded slow-growing bacteria, identified as Salmonella typhi. Prolonged treatment with 2 antimicrobial agents resulted in resolution of skin rash and normalization of laboratory results.
Conclusions: We describe an IL-12Rβ1 deficient patient with a progressive inflammatory process with a unique immune dermatological manifestation which was probably triggered by an unexpected pathogen, Salmonella typhi. This patient’s case demonstrates the need for invasive procedures to identify an infectious etiology when routine cultures and serology tests are negative.
Statement of novelty: In this case report, we describe a unique presentation of infection with Salmonella typhi in a patient with IL-12Rβ1 deficiency, manifesting with bouts of leucocytoclastic vasculitis. We also report in the same patient, recurrent infection with an unusual pathogen, Kocuria kristinae. Both phenomena have not been reported in such constellation, and we believe this to be a useful and important description that could alert physicians, immunologists, and pediatricians alike to such manifestations. Further, it may help in a rapid and successful diagnosis, therefore benefiting such patients.
Introduction
Mendelian susceptibility to mycobacterial disease syndrome (MSMD) encompasses several genetic defects involving the interleukin-12/interferon (IFN) γ axis. Nine different autosomal genes (IFNGR1, IFNGR2, STAT1, IL12B, IL12RB1, IRF8, NEMO, and CYBB) have been described. Interleukin-12 receptor beta 1 (IL-12Rβ1) deficiency is the most common form of MSMD. This syndrome is characterized by susceptibility to intracellular infections mainly with mycobacteria, some weakly virulent mycobacteria such as the bacille Calmette-Guérin, and Salmonella species. Salmonellosis occurs in more than half of affected patients, and while different species can be involved, most are non-typhoid type. Severe morbidity has been reported mainly with extra intestinal manifestations such as lymphadenopathy, septicemia, or recurrent infection with non-typhoid Salmonellae (De Jong et al. 1998; Dorman and Holland 2000). Endovascular involvement of blood vessels during the course of the disease is known but immune phenomena, such as leukocytoclastic skin vasculitis, without direct infection is extremely rare; such a case was previously described in 1 Tunisian and 3 Turkish patients (Kutukculer et al. 2006; Sanal et al. 2006; Filiz et al. 2014; Khamassi et al. 2015). We report here a patient with IL-12Rβ1 deficiency presenting with unusual infections and prolonged intermittent episodes of fever and cutaneous leukocytoclastic vasculitis, which were probably triggered by a Salmonella typhi lymphadenitis.
Patient description
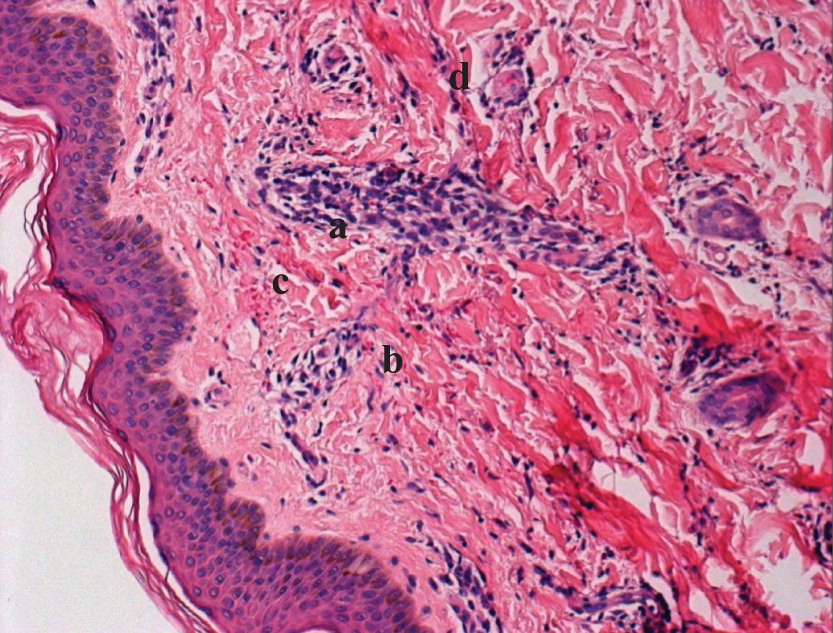
Our patient is an 11 year old male, born to consanguineous parents of Bedouin origin. The patient has been studied and reported previously along with other family members with IL-12Rβ1 deficiency (Ling et al. 2016). He was diagnosed as part of family screening due to an index case. He has 3 family members who were diagnosed with the same mutation, 1 asymptomatic and 2 cousins who had severe infections. One succumbed to a fatal atypical mycobacteria infection, the second survived several Salmonella infections and is now an adult, with a long period of being free of infections. On his first hospitalization with fever, blood cultures were positive for Kocuria kristinae, an unusual pathogen; he was treated and recovered completely only to return a year later with fever without any other symptoms. Blood cultures yielded, again, Kocuria kristinae (Table 1). After a long period in which he was free of symptoms, he was admitted several times to our department with bouts of high fever and rash appearing on his lower extremities, resembling Henoch Schonlein Purpura. Extensive infectious, rheumatologic, and hematologic workup with numerous blood cultures, serologic tests as well as PCR studies of tissue and body fluids did not yield any evidence for infectious etiology. His blood work showed positive ANA with a low titer, and a positive Coombs test. Because of his immunodeficiency, on each occasion, he was treated with broad spectrum antibiotics until cultures returned negative and he was discharged. He appeared well during these episodes and did not have any gastrointestinal or respiratory manifestations, and no other systemic manifestations such as malaise, pain, or other symptoms. On physical examination the only positive finding was progressive enlargement of his spleen. Biopsy of the skin lesions demonstrated a perivascular and interstitial mixed cell infiltrate in the upper and deep dermis, with nuclear dust and foci of extravasation, suggestive of leukocytoclastic vasculitis (Figure 1). Immunofluorescence stains were positive for IgM, C3, and fibrinogen in blood vessel walls. Due to lack of evidence of active infection, alongside positive ANA and positive direct Coombs test, an autoimmune lupus-like photosensitive disease was diagnosed (Ling et al. 2016).
Table 1:
Figure 1:
During the last episode, an abdominal ultrasound study showed significant enlargement of abdominal lymph nodes. We proceeded to obtain a CT-guided lymph node biopsy (Figure 2). Culture from biopsy material yielded a slow-growing bacteria, which was identified as Salmonella typhi.
Figure 2:

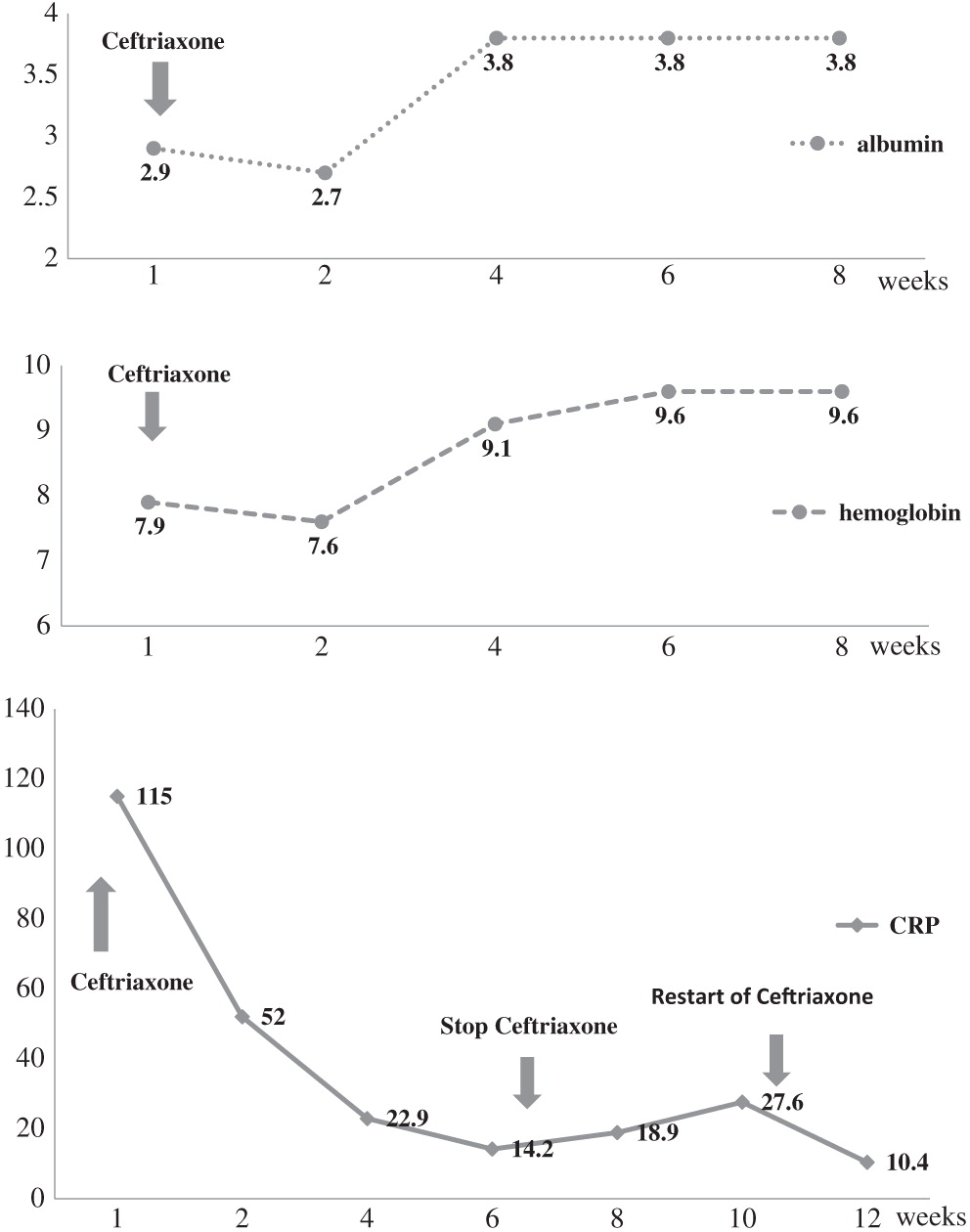
During this period, laboratory indices showed progressive microcytic anemia (hemoglobin 7.2 g/dL, mean corpuscular volume 68 fL), hyponatremia and hypoalbuminemia, elevated C-reactive protein (CRP), and normal white blood cell counts with normal differential (Table 1).
The patient received a combination of parenteral ceftriaxone with oral azithromycin for an initial period of 4 weeks. His laboratory test results improved dramatically, but upon cessation of treatment, inflammatory markers and rash re-emerged. We therefore resumed the same treatment. The patient’s inflammatory indices improved and skin manifestations resolved. However, following a short cessation of therapy due to non compliance by the family, the child again experienced a flare of the vasculitis rash and a rise of CRP. We decided to continue his antibiotic therapy for another 4 weeks which resulted in a remarkable improvement; his spleen size receded significantly, he started to gain weight and all laboratory indices improved (Figure 3).
Figure 3:
Discussion
Vasculitis may be associated with infection, autoimmune diseases, immunization as well as medications. Conversely, patients with an inflammatory disease involving vasculitis may develop infection, which sometimes mimics relapse of the disease. Therefore, such events pose a challenge to the physician caring for an immune deficient patient. Some pathogens are associated with several types of vasculitis (e.g., HIV), whereas others induce a typical vasculitis syndrome (Belizna et al. 2009). The association of enteric pathogen infection with immune phenomenon has led to the suggestion that the adaptive immune response to infection has an auto-immune component (Toivanen et al. 1987; Soloski and Metcalf 2007). In the case presented here, a patient with IL-12Rβ1 deficiency showed a presumed autoimmune phenomenon, which after a considerable period of time, proved to be infectious related. The culprit agent, Salmonella typhi, did not present in any of the common presentations involving the gastrointestinal tract, but rather as recurrent, self-limited, bouts of fever and vasculitic rash. We reviewed the literature describing infections and other manifestations in patients with MSMD and IL-12Rβ1 deficiency in particular, and found that the vast majority of Salmonellae infections are of the non-typhi species. Salmonella typhi was found in 3 of 88 patients (de Beaucoudrey et al. 2010). The very few reports describing vasculitic rash with infections, were associated with mycobacteria, and Salmonella enteritidis (Kutukculer et al. 2006; Sanal et al. 2006; Filiz et al. 2014; Khamassi et al. 2015). This may suggest that in IL-12Rβ1 deficient patients this is a rare but pathognomonic presentation. The mechanism responsible for such a phenomenon is not entirely understood, since secretion of IL-12 resulting in IFNγ release would promote the activity of T cells, and in some autoimmunity models, this is a necessary part of the auto-inflammatory response (Zundler and Neurath 2015). It is possible that the constant inflammatory state in these patients due to an inability to clear infections is, by itself, a promoting factor for autoimmune phenomenon.
Due to the nature of the immune defect involving impaired immune clearance mechanisms, the pathogen being an intracellular bacteria and it’s propensity to dwell in the reticuloendothelial system, treatment of such patients is often challenging. Our case shows that therapy should probably include at least 2 antimicrobial agents, with one of them having an intracellular effect and for a prolonged period, much longer than any standard therapy protocol, in an effort to prevent persistent or relapsing infection. In our patient, any interruption in therapy resulted in recurrence of the disease. Although clinical symptoms resolved fairly quickly, it took as long as 3 months of treatment to reach normal levels of inflammatory makers and blood counts.
It is of interest that this patient had bacteremia with Kocuria kristinae on 2 different occasions. This is an unusual pathogen which is not common in healthy children, but rather found in secondary immunocompromised patients (e.g., patients with cancer or those with complicated diabetes prone to infections) or patients with long standing indwelling catheters (e.g., intensive care unit), where it is known to cause endocarditis (Ahmed et al. 2014). A recent article described a series of cases with the pathogen, where most of the patients were premature newborns and 1 child with leukemia (Chen et al. 2015). However, it has not been described in patients with MSMD to date.
Our report suggests a role for Salmonella typhi as a trigger for vasculitis in patients with immunodeficiency. We also report infections with Kocuria kristinae, an unusual and, to our knowledge, a pathogen not reported yet in this group of patients. It appears that in immunodeficient patients with vasculitic rash, failure to retrieve pathogens by routine tests should prompt a more invasive approach to identify an infectious cause.
REFERENCES
Ahmed N.H., Biswal I., Roy P., and Grover R.K.2014. Kocuria kristinae, an unusual pathogen causing opportunistic infections in patients with malignancy. Indian J. Med. Microbiol.32(4):456–458.
Belizna C.C., Hamidou M.A., Levesque H., Guillevin L., and Shoenfeld Y.2009. Infection and vasculitis. Rheumatology.48(5):475–482.
Chen H.M., Chi H., Chiu N.C., and Huang F.Y.2015. Kocuria kristinae: A true pathogen in pediatric patients. J. Microbiol. Immunol. Infect.48(1):80–84.
de Beaucoudrey L., Samarina A., Bustamante J., Cobat A., Boisson-Dupuis S., Feinberg J., Al-Muhsen S., Jannière L., Rose Y., de Suremain M., Kong X.F., Filipe-Santos O., Chapgier A., Picard C., Fischer A., Dogu F., Ikinciogullari A., Tanir G., Al-Hajjar S., Al-Jumaah S., Frayha H.H., AlSum Z., Al-Ajaji S., Alangari A., Al-Ghonaium A., Adimi P., Mansouri D., Ben-Mustapha I., Yancoski J., Garty B.Z., Rodriguez-Gallego C., Caragol I., Kutukculer N., Kumararatne D.S., Patel S., Doffinger R., Exley A., Jeppsson O., Reichenbach J., Nadal D., Boyko Y., Pietrucha B., Anderson S., Levin M., Schandené L., Schepers K., Efira A., Mascart F., Matsuoka M., Sakai T., Siegrist C.A., Frecerova K., Blüetters-Sawatzki R., Bernhöft J., Freihorst J., Baumann U., Richter D., Haerynck F., De Baets F., Novelli V., Lammas D., Vermylen C., Tuerlinckx D., Nieuwhof C., Pac M., Haas W.H., Müller-Fleckenstein I., Fleckenstein B., Levy J., Raj R., Cohen A.C., Lewis D.B., Holland S.M., Yang K.D., Wang X., Wang X., Jiang L., Yang X., Zhu C., Xie Y., Lee P.P., Chan K.W., Chen T.X., Castro G., Natera I., Codoceo A., King A., Bezrodnik L., Di Giovani D., Gaillard M.I., de Moraes-Vasconcelos D., Grumach A.S., da Silva Duarte A.J., Aldana R., Espinosa-Rosales F.J., Bejaoui M., Bousfiha A.A., Baghdadi J.E., Ozbek N., Aksu G., Keser M., Somer A., Hatipoglu N., Aydogmus C., Asilsoy S., Camcioglu Y., Gülle S., Ozgur T.T., Ozen M., Oleastro M., Bernasconi A., Mamishi S., Parvaneh N., Rosenzweig S., Barbouche R., Pedraza S., Lau Y.L., Ehlayel M.S., Fieschi C., Abel L., Sanal O., and Casanova J.L. 2010. Revisiting human IL12 R B1 deficiency: A survey of 141 patients from 30 countries. Medicine (Baltimore).89:381–402.
De Jong R., Altare F., Haagen I.-A., Elferink D.G., de Boer T., van Breda Vriesman P.J.C., Kabel P.J., Draaisma J.M.T., van Dissel J.T., and Kroon F.P.1998. Severe mycobacterial and Salmonella infections in interleukin-12 receptor-deficient patients. Science. 280:1435–1438.
Dorman S.E. and Holland S.M.2000. Interferon-gamma and interleukin-12 pathway defects and human disease. Cytokine Growth Factor Rev.11:321–333.
Filiz S., Kocacik Uygun D.F., Verhard E.M., van Dissel J.T., Uygun V., Bassorgun C., Bingol A., Yegin O., and van de Vosse E.2014. Cutaneous leukocytoclastic vasculitis due to Salmonella enteritidis in a child with interleukin-12 receptor beta-1 deficiency. Pediatr. Dermatol.31(2):236–240.
Khamassi I., Ben Ali M., Ben Mustapha I., Barbouche M.R., Bejaoui M., Bouyahia O., and Gandoura N.2015. Salmonella enteritidis inducing cutaneous leucocytoclasic vasculitis: An unusual complication in a patient with an interleukine-12 receptor beta-1 deficiency. Tunis Med.93(5):328–329.
Kutukculer N., Genel F., Aksu G., Karapinar B., Ozturk C., Cavusoglu C., Casanova J.L., and Fieschi C.2006. Cutaneous leukocytoclastic vasculitis in a child with interleukin-12 receptor beta-1 deficiency. J. Pediatr.148(3):407–409.
Ling G., Ling E., Broides A., Poran Feldman H., Levy J., Garty B.Z., and Nahum A.2016. IL-12 receptor 1β deficiency with features of autoimmunity and photosensitivity. Autoimmunity. 49(3):143–146.
Sanal O., Turul T., De Boer T., Van de Vosse E., Yalcin I., Tezcan I., Sun C., Memis L., Ottenhoff T.H., and Ersoy F.2006. Presentation of interleukine-12/-23 receptor β1 deficiency with various clinical symptoms of Salmonella infections. J. Clin. Immunol.26(1):1–6.
Soloski M.J. and Metcalf E.S.2007. Salmonella as an inducer of autoimmunity. EcoSal Plus.2(2).
Toivanen A., Lahesmaa-Rantala R., Meurman O., Sappinen O., Kosunen T., Yazici H., Yurdakul S., Ozbakir F., and Müftüoglu A.1987. Antibodies against Yersinia, Campylobacter, Salmonella, and Chlamydia in patients with Behçet’s disease. Arthritis Rheum.30(11):1315–1317.
Zundler S. and Neurath M.F.2015. Interleukin-12: Functional activities and implications for disease. Cytokine Growth Factor Rev.26(5):559–568.
Information & Authors
Information
Published In
LymphoSign Journal
Volume 4 • Number 1 • March 2017
Pages: 25 - 29
History
Received: 27 October 2016
Accepted: 29 November 2016
Accepted manuscript online: 11 December 2016
Version of record online: 11 December 2016
Copyright
© 2017.
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
Amarilla B.Mandola, ArnonBroides, and AmitNahum. 2017. Salmonella typhi infection causing prolonged chronic illness and cutaneous leucocytoclastic vasculitis in a patient with IL-12 receptor β1 deficiency. LymphoSign Journal.
4(1): 25-29. https://doi.org/10.14785/lymphosign-2016-0013
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
