The psychological effects of systemic lupus erythematosus: the imitator of aging
Abstract
Objectives: To assess the psychological effects of systemic lupus erythematosus (SLE), including perception of aging, in a cohort of participants who were either diagnosed with SLE or had an affected family member.
Methods: Over a period of 1 year, we conducted once-monthly face-to-face interviews with 12 participants. The participants were from 4 related families and include 7 females and 5 males. Three participants had a confirmed diagnosis of SLE. Spouses were also included in this study to assess transitivity of the psychological signs of SLE. Responses to structured interview questions were analyzed to assess the perception of aging.
Results: The major complaints in participants diagnosed with SLE were pain and psychological stress. Nephrotic syndrome, urinary tract infection, weight disorders and increased need for psychosocial support were common in the participants’ medical history. Qualitative analysis of questionnaires completed by participants with SLE revealed a correlation of “feeling old” with the non-resolution of health complaints. Family members who did not have SLE also reported “feeling old”. Complaints of stress, anxiety, nervousness and lack of enjoyment of life were common in those who were diagnosed with SLE, as well as those who were not. All spouses reported experiencing digestive disorders, hemorrhoids as well as various phobias, regardless of whether their partners had a confirmed SLE diagnosis.
Conclusions: In this study, we found that participants with SLE or those who had a close family member with SLE displayed psychological signs of aging. All participants had a predisposition to anxiety, while spouses developed various phobias.
Statement of novelty: We show that individuals with SLE and close family members have an increased self-perception of aging.
Introduction
Systemic lupus erythematosus (SLE) is a chronic inflammatory disease that occurs when components of the immune system attack the body’s own tissues and organs. While the etiology is not completely understood, it is known that genetics, environmental factors and hormones play a clear role. Autoantibody production and decreasing testosterone or estrogen levels can trigger the disease (Boodhoo et al. 2016; Braga et al. 2019). Psychological stress, ultraviolet rays, infections and some drugs (hydralazine, isoniazid, procainamide, diphenylhydantoin) are also known triggers (Moses et al. 2005; Seawell and Danoff-Burg 2005; Mendelson 2006; Monaghan et al. 2007; Danoff-Burg and Friedberg 2009; Philip et al. 2009).
Given the complexity of SLE, its clinical presentation may imitate other diseases, including autoimmune thyroid disease, rheumatoid arthritis, celiac disease, Sjögren’s syndrome, myasthenia gravis, scleroderma, antiphospholipid syndrome, polymyositis, dermatomyositis, and scleroderma.
The most common clinical symptoms in patients with SLE are musculoskeletal problems. Joint pain, pain in the wrist, and knee pain are among the most frequently reported symptoms. Myopathy, osteonecrosis, and arthritis are also reported. Approximately 5%–10% of patients with SLE have antibodies to citrullinated peptides, and these antibodies are associated with erosive arthritis (Budhram et al. 2014; Di Matteo et al. 2019; Jung et al. 2019; Metry et al. 2019; Malekan and Kontzias 2020). Dermatological manifestations are another clinical symptom and include malar rash, discoid rash, livedo reticularis, lupus profundus, vasculitic purpura, urticaria, and telangiectasias. Although alopecia with patchy loss and butterfly rash are among the prominent signs of this disease, it is not sufficient for definitive diagnosis (Cojocaru et al. 2011). Lupus nephritis occurs in most cases of SLE (Zheng et al. 2019). Gastrointestinal findings, as well as cardiac and vascular manifestations are also common. Takayasu’s arteritis and Raynaud’s phenomenon occur in a small majority of SLE patients. Similarly, keratoconjunctivitis sicca is an ocular manifestation that has also been reported. Obstetric manifestations may cause spontaneous abortions and fetal retardation. One of the most important findings in SLE patients are endocrine manifestations, including thyroid dysfunction, of which middle-aged and older women are at higher risk (Wang et al. 2019). Similarly, lymphopenia, leukopenia and hematologic manifestations often occur as well (Jung et al. 2019). Pulmonary manifestions include pleurisy, dyspnea, hemoptysis and thromboembolic diseases (Kokosi et al. 2019). Neurological effects have also been reported. Studies have shown that the incidence of antiphospholipid antibodies in SLE patients is high (Ben-Menachem 2010).
SLE causes psychological problems associated with depression and anxiety, causing psychological behavior patterns (Moses et al. 2005; Mendelson 2006; Monaghan et al. 2007; Budhram et al. 2014). Anecdotal reports suggest that SLE is associated with high vulnerability and patients can experience emotional and psychological issues, especially during the treatment process (Iverson 1995; Druley et al. 1997; Santoantonio et al. 2006; Schattner et al. 2008; Andrews et al. 2009; Shucard et al. 2011). Acute confusional state and psychosis occurs less frequently than other symptoms (Hanly et al. 2019). Certain neurological dysfunctions may also result in a decrease in the individual’s ability to focus. Visual-auditory hallucination in SLE patients can result in psychosis (Kang and Mok 2019). Cognitive dysfunction such as psychomotor speed or memory disorders, including pain and sleep problems, may also occur. Together, the combination of these symptoms can cause mood disorders, and are associated with manic or depressive episodes (Ainiala et al. 2001; Meszaros et al. 2012). Anxiety is more likely to occur in those with SLE than in normal healthy individuals. Obsessive-compulsive disorder and panic disorders have also been reported (Papadaki et al. 2019). Fatigue, irritability and sadness are also prevalent. All these symptoms and factors decrease the quality of life of patients with SLE.
Neuropsychological effects adversely affect the behavior of SLE patients. These negative psychological behavior patterns can become even more pronounced during aging, a process defined as an individual’s cognitive, mental, psychological, psychosocial, physical, biological and social decline. Palliative diseases have been found to affect the self-perception of aging. According to clinically determined findings, the psychological and physical effects of disease in palliative patients affects self-perception of aging (Richardson 2002; Rodriguez et al. 2007; Hupcey et al. 2009; McLaughlin et al. 2011), and decreases quality of life. These effects are similar to the neuropsychological symptoms of SLE, and raises questions of a possible association between SLE and self-perception of aging.
To date, there are no convincing studies on the pathological causes of behavior patterns that SLE patients experience. Further, the psychological effect of SLE on self-perception of aging has not been investigated. Here, we sought to assess the perception of aging in 4 related families and spouses who were directly or indirectly affected by SLE.
Methods
Patients
Twelve participants were enrolled in this study. Participants’ consent for this research was obtained; all participants were informed that involvement was voluntary and that they could withdraw from the study at any time. All names were coded to protect privacy.
Interview questions
Research questionnaires (Appendix 1) were administered once-monthly with family members via face-to-face interaction for a period of 1 year. Qualitative research methodology and multiple case designs were adopted in this study, and structured interviews, data collection and observation techniques used (Gerring 2004). The predetermined questions were asked to all participants in the same order (Gall et al. 1996). As interview questions are important for revealing an identified phenomenon, an extended literature review was conducted on how the perception of aging should be determined (Billino and Pilz 2019; Fougner et al. 2019; Gire 2019; Gurera and Isaacowitz 2019; Hooker et al. 2019; Parish et al. 2019; Smith and Bryant 2019; Srivarathan et al. 2019). At the end of this review, the questions in Appendix 1 were created.
Semi-structured questions were directed to each participant and each session was recorded so that it could be systematically examined at a later time. To determine the consistency of the data and whether the questions had the same meaning for each participant, a pre-test was conducted with a sample of 48 individuals (22 males, 26 females; ages ranging from 28 to 64) with different demographic characteristics. As a result of this pre-test, the questions were determined to be valid and reliable.
Analysis of qualitative data was performed using MAXQDA and Voyant Tools programs which include concept mapping techniques. Data analysis was performed by conceptualization, classification, coding and component analysis (Spiers and Riley 2019), and was evaluated by 2 academicians who were not involved in the study field to minimize the risk of systematic errors. The evaluations were compared, the differences analyzed and the common results reported.
Coding is the process of revealing concepts appropriate to the meaning of the sentences in the data set (Mihas 2019). During this process, the words (part of a participants’ response) are highlighted in the sentence, and word meanings are examined as a whole. The concepts introduced by coding are classified according to the topics. The concepts connected with each other as meaning and subject are combined (Riley et al. 2019). For instance, the relationship between the responses given to the questions “Could you tell us about your physical, psychological and mental complaints?” and “How do you feel when your complaints occur?” were evaluated by comparing the medical reports. After the interviews were completed, the participants’ thoughts on self-perception of aging were analysed. Q6 measured the individual’s perception of aging related to the disease and Q7 measured the perception of aging related to the complaints of the individual. Finally, Q8 was specifically directed to reveal the effects of negative symptoms of SLE on spouses after marriage. All these questions and responses were classified after recording. The themes, topics, and classification that were created were re-evaluated at the end of the study to ensure integrity of the subject.
Results
The 7 female and 5 male participants were members of 4 related families living in the province of Adana, Turkey (Figure 1). The maternal grandmother (Pt L), daughter (Pt Y), and grand-daughter (Pt X1) were clinically diagnosed with SLE. Two daughters (Pt X, Z) and 3 grand-children (Pt X2, Y1, Y2) did not have SLE. Similarly, none of the spouses (Pt A, B, C, D) had SLE. Participant demographics are shown in Table 1. None practiced regular exercise. Each revealed that their family relations were good, there were no smoking habits and alcohol was rarely consumed. None of the participants had suffered a major loss or traumatic event in their history.
Figure 1:
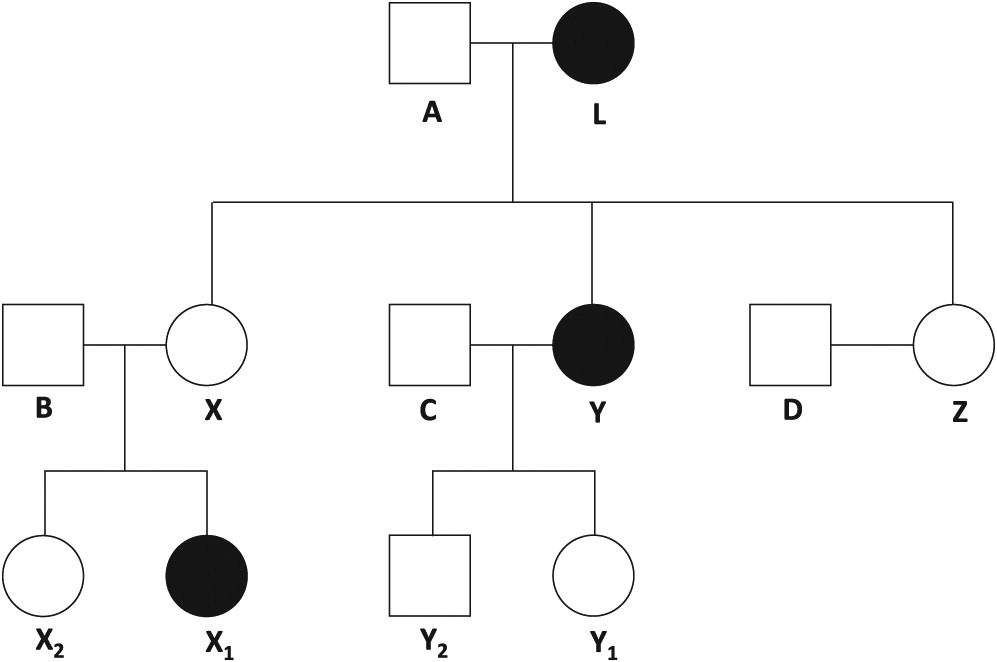
Table 1:
Review of medical charts and results of the questionnaires revealed that, although Pt X, X2, Y1 and Z did not have a clinical diagnosis of SLE, they had similar complaints and disorders as the family members with SLE (Table 2). Further clinical assessment (anti-nuclear antibody, anti-dsDNA, cryoglobin and complement c3 testing) did not support a diagnosis of SLE in these participants. All participants, with the exception of Pt Y2, had severe anxiety and phobia predisposition (Table 3).
Table 2:
a
Adapted from self-reported knowledge and past clinical reports.
b
Post-nuptial syndromes.
Table 3:
a
Adapted from self-reported knowledge and past clinical reports.
b
Post-nuptial syndromes.
The participants with confirmed SLE were asked about their diagnosis of SLE and their perception of aging. Each believed that there was a relationship between aging and the non-resolution of complaints. One participant’s response was: “My complaints are increasing due to my illness. I think I’m getting old.”. Another participant stated: “My life was ruined because of this disease. I have constant joint pain. As my pains increase, I remember the complaints of old people. I think I’m getting old.” All participants indicated that they preferred to give up struggling with their diseases and disorders, as their complaints could not be solved despite visits to the doctor. Participants often felt this way when the pain became unbearable. Some statements from the participants were as follows: “This disease is killing me day by day. Treatment and medications are insufficient. I feel old. This desperation overwhelms me.”, “My husband is my biggest supporter. But he is not able to do anything. I have all the complaints of the elderly people around me. I am not different from them.”
When the same questions were asked to the female participants who had not been diagnosed with SLE, but had symptoms of this disease, they stated that they were very anxious about having SLE. Statements include: “I am very afraid of lupus. After all, this disease seems to be taking over the whole family. We have the same complaints as my sister and my mother. From time to time we talk among ourselves. We’re evaluating my mother’s and sister’s complaints. I worry about them.”
The husbands of Pt L, X, Y, and Z (Pt A, B, C and D, respectively) were included in this study to assess the effects of SLE on psychological transitivity. Psychological transitivity is the ability of individuals to subconsciously imitate the psychological behaviour patterns of physical states and movements, including diseases, such as SLE (Dai 2017). In this qualitative study conducted with husbands of the participants, we found that each spouse experienced psychological problems; their phobia susceptibility increased, and they did not experience these complaints before their marriage (Table 3). Some responses from the participants were as follows: “I did not have psychological problems before I got married. I love my wife. But I also feel the same pains from time to time because of her constant pains. I think I’m starting to look like her.”, “Even when I was in the army, I didn’t have that much stress. Everything was fine in the first years we got married. Later, my wife’s joint pain began to exacerbate. Pain in the kidneys and headaches gradually gained momentum. Going to a doctor continuously has worn me out. When I take her to the doctor, I go too. What’s the difference between us? I think this disease is contagious. I also experience her complaints from time to time.”
Pt A, B, C and D were noted to have digestive and stomach disorders, as well as hemorrhoids (Table 3). Each stated that their life quality was decreased, due to constant medical check-ups. Some of the responses to the interview questions include: “Going to the doctors to check-up continuously and seeing that there is no solution reduces your joy of life. Imagine that your partner is melting away in front of you, has constant pain, please think about it. My mind is always with her. Your quality of life is completely under zero.”, “After my wife’s pain started, I started to experience a stomach pain. I am constantly getting constipated. When I went to the doctor, he said it was psychological. This affects my life in a negative way.”
Discussion
In this study, we found that the psychological effects of SLE increased the self-perception of aging, with the participants reporting themes of “feeling old”. Individuals with SLE related their symptoms in a similar way to the physical and psychological decline that occurs with aging. This aspect may be an important neuropsychological determinant in SLE. Female participants who were not diagnosed with SLE also reported the same or similar complaints as their family members who did have an SLE diagnosis, including tingling in arms, legs, feet and shoulder, arthritis pain, sadness, stress, crying (emotional incontinence), anxiety, nervousness, the status quo of unhappiness, not enjoying life, feeling old. Since SLE is more common in females than males, it is important to explore whether female relatives of affected individuals may have SLE.
We found that the complaints of Pt L, X1 and Y, who had a diagnosis of SLE, were pain and psychological based. Nephrotic syndrome, urinary tract infection, weight disorders, and the need for psychosocial support were common in the medical history of these participants. While the other participants did not have SLE, their similar health complaints creates an important perception about SLE. This perception causes psychological problems and affected the spouses in this study negatively.
Various phobias were noted in spouses of the participants: Pt A: aichmophobia, pharmacophobia, iatrophobia; Pt B: pteromerhanophobi, claustrophobia; Pt C: hemophobia, carnophobia; Pt D: atychiphobia. These psychological disorders emerged after marriage, and may be associated with long-term stress and anxiety (Fox et al. 2005). Furthermore, the spouses each complained of digestive and stomach disorders as well as hemorrhoids. Together these demonstrate the negative impact of SLE on the psychological and medical problems that occur after marriage to a person with SLE.
The pain imbalance experienced by SLE patients should be evaluated in terms of neuropsychological aspects, and recommendations should be made to treat the psychological problems experienced by spouses of patients with chronic diseases.
This study had some limitations, including possible prejudices of the participants. Presenting the views and situations of the participants with predetermined questions limited the generalizability of the results. Thus, it would be important to perform such studies involving participants with different demographic characteristics. It may be of interest to repeat this study with palliative patients and their spouses, since palliative diseases include chronic neurological diseases (such as dementia). This would help to better understand self-perception of aging and psychological transitivity in these diseases (Anneser et al. 2018).
Conclusion
Our findings showed that patients with SLE had increased self-perception of aging, and were predisposed to anxiety and phobias. Close family members of individuals with SLE were found to be under psychological threat.
REFERENCES
Ainiala H., Loukkola J., Peltola J., Korpela M., and Hietaharju A. 2001. The prevalence of neuropsychiatric syndromes in systemic lupus erythematosus. Neurology. 57(3):496–500.
Andrews N.R., Chaney J.M., Mullins L.L., Wagner J.L., Hommel K.A., and Jarvis J.N. 2009. The differential effect of child age on the illness intrusiveness–parent distress relationship in juvenile rheumatic disease. Rehabil. Psychol. 54(1):45–50.
Anneser J., Arenz V., and Borasio G.D. 2018. Neurological symptoms in palliative care patients. Front. Neurol. 9:275.
Ben-Menachem E. 2010. Systemic lupus erythematosus: A review for anesthesiologists. Anesth. Analg. 111(3):665–676.
Billino J. and Pilz K.S. 2019. Motion perception as a model for perceptual aging. J. Vis. 19(4):3.
Boodhoo K.D., Liu S., and Zuo X. 2016. Impact of sex disparities on the clinical manifestations in patients with systemic lupus erythematosus: A systematic review and meta-analysis. Medicine. 95(29):e4272.
Braga J., Rothwell R., Oliveira M., Rodrigues D., Fonseca S., Varandas R., and Ribeiro L. 2019. Choroid thickness profile in patients with lupus nephritis. Lupus. 28(4):475–482.
Budhram A., Chu R., Rusta-Sallehy S., Ioannidis G., Denburg J.A., Adachi J.D., and Haaland D.A. 2014. Anti-cyclic citrullinated peptide antibody as a marker of erosive arthritis in patients with systemic lupus erythematosus: A systematic review and meta-analysis. Lupus. 23(11):1156–1163.
Cojocaru M., Cojocaru I.M., Silosi I., and Vrabie C.D. 2011. Manifestations of systemic lupus erythematosus. Maedica. 6(4):330–336.
Dai J. 2017. Using tests of transitivity to evaluate psychological models of intertemporal choice for individuals: Reply to Scholten (2017). Decision. 4(2):127–130.
Danoff-Burg S. and Friedberg F. 2009. Unmet needs of patients with SLE. Behav. Med. 35(1):5–13.
Di Matteo A., Isidori M., Corradini D., Cipolletta E., McShane A., De Angelis R., Filippucci E., and Grassi W. 2019. Ultrasound in the assessment of musculoskeletal involvement in systemic lupus erythematosus: State of the art and perspectives. Lupus. 28(5):583–590.
Druley J.A., Stephens M.A.P., and Coyne J.C. 1997. Emotional and physical intimacy in coping with lupus: Women’s dilemmas of disclosure and approach. Health Psychol. 16(6):506–514.
Fougner M., Bergland A., Lund A., and Debesay J. 2019. Aging and exercise: Perceptions of the active lived-body. Physiother. Theory Pract. 35(7):651–662.
Fox N.A., Henderson H.A., Marshall P.J., Nichols K.E., and Ghera M.M. 2005. Behavioral inhibition: Linking biology and behavior within a developmental framework. Annu. Rev. Psychol. 56(1):235–262.
Gall, M.D., Barg, W.R., and Gall, J.P. 1996. Educational research: An introduction. 6th ed. White Plains, NY, USA: Longman.
Gerring J. 2004. What is a case study and what is it good for? Am. Polit. Sci. Rev. 98(2):341–354.
Gire, J.T. 2019. Cultural variations in perceptions of aging. In Cross‐cultural psychology: Contemporary themes and perspectives. pp. 216–240.
Gurera J.W. and Isaacowitz D.M. 2019. Emotion regulation and emotion perception in aging: A perspective on age-related differences and similarities. Prog. Brain Res. 247:329–351.
Hanly J.G., Li Q., Su L., Urowitz M.B., Gordon C., Bae S.C., Romero-Diaz J., Sanchez-Guerrero J., Bernatsky S., Clarke A.E., Wallace D.J., Isenberg D.A., Rahman A., Merrill J.T., Fortin P.R., Gladman D.D., Bruce I.N., Petri M., Ginzler E.M., Dooley M.A., Steinsson K., Ramsey-Goldman R., Zoma A.A., Manzi S., Nived O., Jonsen A., Khamashta M.A., Alarcón G.S., van Vollenhoven R.F., Aranow C., Mackay M., Ruiz-Irastorza G., Ramos-Casals M., Lim S.S., Inanc M., Kalunian K.C., Jacobsen S., Peschken C.A., Kamen D.L., Askanase A., Theriault C., and Farewell V. 2019. Psychosis in systemic lupus erythematosus: Results from an international inception cohort study. Arthritis Rheumatol. 71(2):281–289.
Hooker K., Mejía S.T., Phibbs S., Tan E.J., and Stevens J. 2019. Effects of age discrimination on self-perceptions of aging and cancer risk behaviors. Gerontologist. 59(Suppl. 1):S28–S37.
Hupcey J.E., Penrod J., and Fogg J. 2009. Heart failure and palliative care: Implications in practice. J. Palliat. Med. 12(6):531–536.
Iverson G.L. 1995. The need for psychological services for persons with systemic lupus erythematosus. Rehabil. Psychol. 40(1):39–49.
Jung U.H., Kwak S.G., Choe J.Y., Lee S.S., and Kim S.K. 2019. The effect of mycophenolate mofetil on non-renal manifestations in systemic lupus erythematosus: Results from Korean Lupus Network registry. J. Korean Med. Sci. 34(27):e185.
Kang D. and Mok C.C. 2019. Management of psychosis in neuropsychiatric lupus. J. Clin. Rheumatol. Immunol. 19(1):9–17.
Kokosi M., Lams B., and Agarwal S. 2019. Systemic lupus erythematosus and antiphospholipid antibody syndrome. Clin. Chest Med. 40(3):519–529.
Malekan, M., and Kontzias, A. 2020. Musculoskeletal manifestations of systemic diseases. In Absolute rheumatology review. Springer, Cham, Switzerland. pp. 425–445.
McLaughlin D., Hasson F., Kernohan W.G., Waldron M., McLaughlin M., Cochrane B., and Chambers H. 2011. Living and coping with Parkinson’s disease: Perceptions of informal carers. Palliat. Med. 25(2):177–182.
Mendelson C. 2006. Managing a medically and socially complex life: Women living with lupus. Qual. Health Res. 16(7):982–997.
Meszaros Z.S., Perl A., and Faraone S.V. 2012. Psychiatric symptoms in systemic lupus erythematosus: A systematic review. J. Clin. Psychiatry. 73(7):993–1001.
Metry A.M., Al Salmi I., Al Balushi F., Yousef M.A., Al Ismaili F., Hola A., and Hannawi S. 2019. Systemic lupus erythematosus: Symptoms and signs at initial presentations. Antiinflamm. Antiallergy Agents Med. Chem. 18(2):142–150.
Mihas, P. 2019. Qualitative data analysis. In Oxford research encyclopedia of education.
Monaghan S.M., Sharpe L., Denton F., Levy J., Schreiber L., and Sensky T. 2007. Relationship between appearance and psychological distress in rheumatic diseases. Arthritis Rheum. 57(2):303–309.
Moses N., Wiggers J., Nicholas C., and Cockburn J. 2005. Prevalence and correlates of perceived unmet needs of people with systemic lupus erythematosus. Patient. Educ. Couns. 57(1):30–38.
Papadaki E., Kavroulakis E., Bertsias G., Fanouriakis A., Karageorgou D., Sidiropoulos P., Papastefanakis E., Boumpas D.T., and Simos P. 2019. Regional cerebral perfusion correlates with anxiety in neuropsychiatric SLE: Evidence for a mechanism distinct from depression. Lupus. 28(14):1678–1689.
Parish A., Kim J., Lewallen K.M., Miller S., Myers J., Panepinto R., and Maxwell C.A. 2019. Knowledge and perceptions about aging and frailty: An integrative review of the literature. Geriatr. Nurs. 40(1):13–24.
Philip E.J., Lindner H., and Lederman L. 2009. Confidence in medical care linked to depression in lupus sufferers. J. Allied Health. 38(2):106–112.
Richardson J. 2002. Health promotion in palliative care: The patients’ perception of therapeutic interaction with the palliative nurse in the primary care setting. J. Adv. Nurs. 40(4):432–440.
Riley S., Brooks J., Goodman S., Cahill S., Branney P., Treharne G., and Sullivan C. 2019. Celebrations amongst challenges: Considering the past, present and future of the Qualitative Methods in Psychology (QMiP) section of the British Psychological Society. Qual. Res. Psychol. 16(3):464–482.
Rodriguez K.L., Barnato A.E., and Arnold R.M. 2007. Perceptions and utilization of palliative care services in acute care hospitals. J. Palliat. Med. 10(1):99–110.
Santoantonio J., Yazigi L., and Sato E.I. 2006. Rorschach characteristics in adolescents with systemic lupus erythematosus. Rorschachiana. 28(1):100–118.
Schattner E., Shahar G., and Abu-Shakra M. 2008. I used to dream of lupus as some sort of creature: Chronic illness as an internal object. Am. J. Orthopsychiatry. 78(4):466–472.
Seawell A. and Danoff-Burg S. 2005. Body image and sexuality in women with and without systemic lupus erythematosus. Sex Roles. 53(11–12):865–876.
Shucard J.L., Lee W.H., Safford A.S., and Shucard D.W. 2011. The relationship between processing speed and working memory demand in systemic lupus erythematosus: Evidence from a visual n-back task. Neuropsychology. 25(1):45–52.
Smith J.L. and Bryant F.B. 2019. Enhancing positive perceptions of aging by savoring life lessons. Aging Mental Health. 23(6):762–770.
Spiers J. and Riley R. 2019. Analysing one dataset with two qualitative methods: The distress of general practitioners, a thematic and interpretative phenomenological analysis. Qual. Res. Psychol. 16(2):276–290.
Srivarathan A., Jensen A.N., and Kristiansen M. 2019. Community-based interventions to enhance healthy aging in disadvantaged areas: Perceptions of older adults and health care professionals. BMC Health Serv. Res. 19(1):7.
Wang Z., Li M., Zhao J., Wang Q., and Zeng X. 2019. 220 Clinical characteristics and remission of patients with systemic lupus erythematosus in China: Results from SLE treatment and research group (CSTAR) registry with a real-time collecting system. Lupus Sci. Med. 6(Suppl. 1):A164.
Zheng X., Xiao Z.X., Hu L., Fang X., Luo L., and Chen L. 2019. Dendritic cell-associated B7-H3 suppresses the production of autoantibodies and renal inflammation in a mouse model of systemic lupus erythematosus. Cell Death Dis. 10(6):1–11.
Appendix 1
Q1—Demographic variables (age, gender, marital status)
Q2—Do you have a Systemic Lupus Erythematosus (Lupus) disease diagnosed by a doctor?
Q3—Could you tell us about your physical, psychological and mental complaints?
Q4—How do you feel when your complaints occur?
Q5—What do you think about the reasons for your complaints?
Q6—Do you think there is a relationship between aging and your disease?
Q7—Do you think there is a relationship between aging and your complaints?
Q8—Doctor-diagnosed diseases of pre-marriage (10 years) and post-marriage, and treatment documents (Medical history).
Information & Authors
Information
Published In

LymphoSign Journal
Volume 7 • Number 1 • March 2020
Pages: 37 - 45
History
Received: 8 October 2019
Accepted: 20 January 2020
Accepted manuscript online: 28 January 2020
Copyright
© 2020.
Authors
Competing Interests
The Author declares that they have no conflict of interest.
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
FahriÖzsungur. 2020. The psychological effects of systemic lupus erythematosus: the imitator of aging. LymphoSign Journal.
7(1): 37-45. https://doi.org/10.14785/lymphosign-2019-0016
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
