Case of 22q11.2 deletion syndrome not identified by TBX1 screening with a positive SCID newborn screen
Abstract
Individuals with 22q11.2 deletion syndrome (22q11.2DS) have an embryological midline fusion defect, which can result in a syndrome including congenital heart disease, cleft palate, hypoparathyroidism, thymic hypoplasia, immunologic abnormalities, and developmental delay. The majority of patients have a 3 megabase deletion, which contains multiple genes, including the T-box transcription factor (TBX1) gene. Definitive diagnosis is made through fluorescent in situ hybridization (FISH) or chromosomal microarray (CMA). Newborn screening (NBS) for severe combined immune deficiency (SCID) via low T-cell receptor excision circles (TRECs) can also identify this population if thymic output is low. Samples from infants who screen positive undergo further testing, which includes a purine profile and TBX1 deletion analysis. Diagnostic follow-up testing is centre-dependent and may not include more definitive testing for 22q11.2DS by FISH or CMA. We report a case of a newborn with 22q11.2DS, detected by low TRECs on the SCID NBS, with a normal screening TBX1 result, who was subsequently found to have a TBX1 gene deletion on follow-up 22q11.2 FISH and CMA. This case highlights the limitations of the TBX1 screening assay and the importance of performing diagnostic testing with FISH and (or) CMA regardless of the initial TBX1 result. It also emphasizes the need for a standardized follow-up testing algorithm across institutions for newborns who screen positive for SCID.
Statement of novelty: To our knowledge, this is the first case to be described in the literature where a newborn with 22q11.2DS with a typical deletion encompassing the TBX1 gene was not identified by initial TBX1 screening, highlighting the limitations of this test as a standalone screening assay.
Background
The most common chromosomal microdeletion disorder identified in children is 22q11.2 deletion syndrome (22q11.2DS), whereby affected individuals are missing a small piece of chromosome 22 containing genes responsible for midline fusion during the embryological period. The syndrome results in a constellation of signs and symptoms, described as DiGeorge or Velocardiofacial Syndrome. Some of the clinical features include congenital heart disease, cleft palate, hypoparathyroidism, thymic hypoplasia, immunologic abnormalities, developmental delay, psychiatric disorders, and distinct facial features (McDonald-McGinn et al. 2015).
The most common deletion responsible for the syndrome, present in 85% of individuals, involves 3 megabases (Mb) in the 22q11.2 chromosomal region (McDonald-McGinn et al. 2013). This region contains 90 known or predicted genes, including the T-box transcription factor (TBX1) gene. The TBX1 gene is implicated in several of the clinical features of the syndrome. Most of the remaining patients have smaller 1.5 Mb deletions, referred to as atypical “nested” deletions (McDonald-McGinn et al. 2015).
Suggestive clinical presentations have traditionally prompted evaluation for 22q11.2DS through the use of fluorescent in situ hybridization (FISH) using specific probes, including TUPLE or N25. Chromosomal microarray (CMA) and multiplex ligation-dependent probe amplification (MLPA) can also be used, particularly to identify smaller nested deletions not detectable by FISH (McDonald-McGinn et al. 2015).
To allow for earlier detection and diagnosis, the inclusion of 22q11.2DS in newborn screening (NBS) panels has been proposed (Pretto et al. 2015). However, routine screening has not yet been implemented. Given that immune dysfunction, specifically low or absent T-cells, is present in some cases of 22q11.2DS, some patients can be identified by NBS for severe combined immune deficiency (SCID), through detection of low T-cell receptor excision circles (TRECs). TRECs are a biomarker of naïve T-cells and their absence signifies low or absent T-cell production (Kwan and Puck 2015). The TREC screen primarily aims to identify forms of SCID; however, it also identifies infants with non-SCID T-cell lymphopenia. The differential for these secondary targets is broad, and includes syndromes such as 22q11.2DS, other combined immune deficiencies, as well as cardiac and gastrointestinal diseases and lymphatic malformations (Dorsey and Puck 2017).
In the last 4 years, SCID NBS has been implemented across North America, in Ontario, the Canadian Maritime provinces, and most American states. In Ontario, term infants (defined as ≥33 weeks gestational age and ≥1500 g) with a TREC level falling below a set cutoff, falling significantly below the normal range, will screen positive for SCID. Further screening, including a purine profile and a quantitative polymerase chain reaction (q-PCR)-based TBX1 deletion analysis to screen for 22q11.2DS, is subsequently performed on the NBS samples from this group of infants. Infants with a screen positive result for SCID are referred for additional investigation. Follow-up testing typically includes a repeat dried blood sample for repeat TREC, TBX1, and purine profile screening. Diagnostic follow-up often includes a complete blood count with a differential, lymphocyte immunophenotyping, testing for 22q11.2DS via FISH or CMA, and consultation with a medical expert. Follow-up testing practices vary across centres.
Herein, we report a case of a newborn with 22q11.2DS detected by low TRECs on the SCID NBS, with a normal screening TBX1 result. A deletion involving the TBX1 gene was subsequently detected on our centre’s standard follow-up 22q11.2 FISH, and by subsequent CMA. This case highlights the limitations of the TBX1 screening assay and the importance of performing diagnostic testing with FISH and (or) CMA regardless of the initial TBX1 result.
Case presentation
A newborn male born after an uncomplicated, non-consanguineous pregnancy was born at 38 weeks gestation with a birth weight of 2390 g. NBS done at 24 hours of life was positive for SCID. Initial screening revealed a low TREC value of 54 copies/3 μL (cutoff: 75, reference interval: 228–2634), normal purine profile and a normal TBX1 analysis with no deletion detected. Upon assessment in our Pediatric Immunology Clinic, he appeared well. Physical examination demonstrated a non-dysmorphic infant with intact palate, palpable lymph nodes, and cardiovascular examination within normal limits. The remainder of the examination was unremarkable. The TREC screening assay was repeated and the value remained low at 51 copies/3 μL on the follow up sample, with a normal purine profile and TBX1 analysis. Additional investigations included a complete blood count with differential and lymphocyte immunophenotyping, which were within normal range.
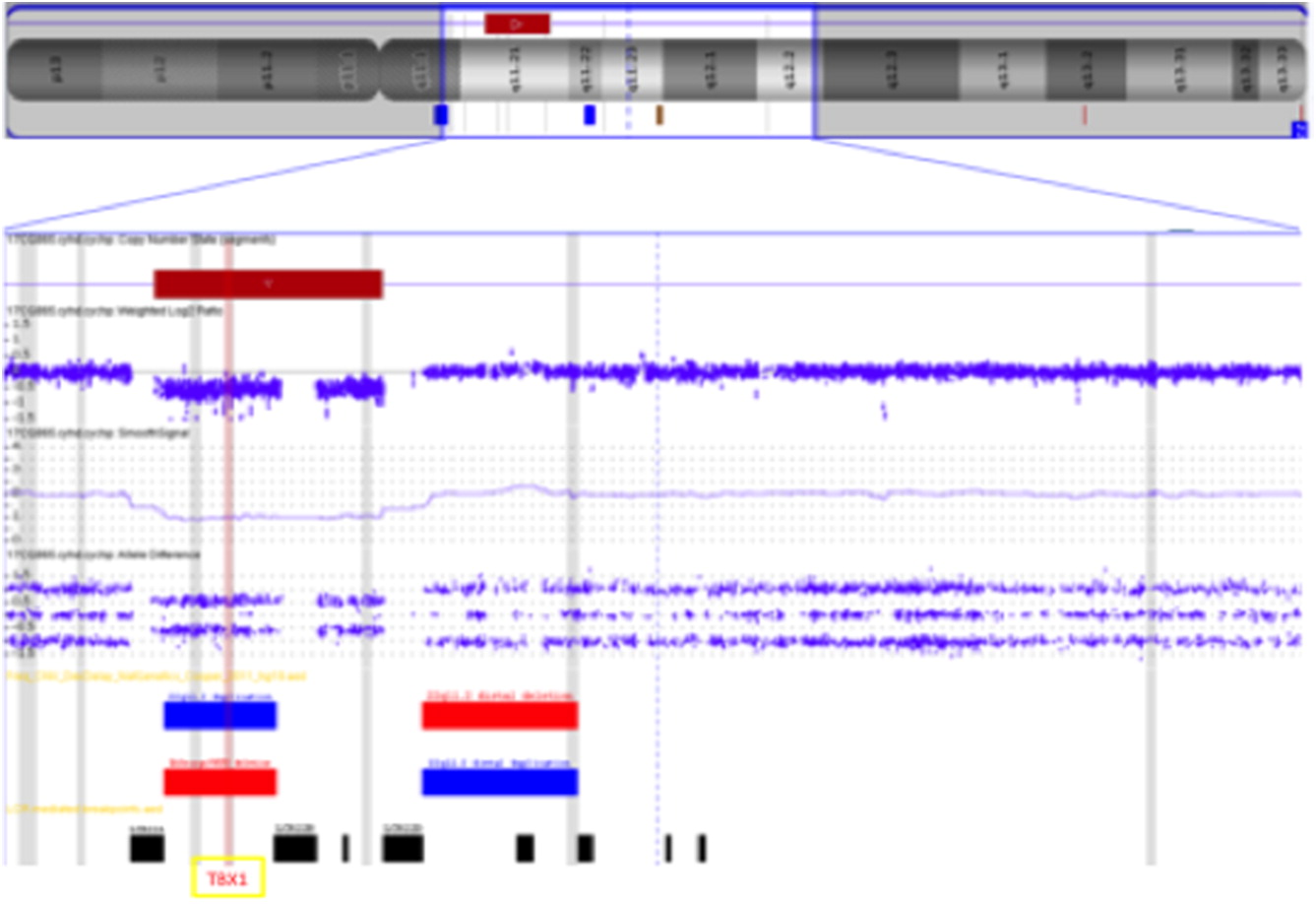
Despite the normal TBX1 screening analysis, a FISH assay to assess for 22q11.2DS was performed as part of the subsequent routine testing protocol at McMaster Children’s Hospital. A deletion in the 22q11.2 region was identified on FISH (Figure 1). A CMA was subsequently performed to further delineate the deletion, which detected a 2.5 Mb microdeletion within the typical 3 Mb region, including the TBX1 gene. This confirmed the diagnosis of 22q11.2DS (Figure 2) for this patient. An echocardiogram was performed, revealing an aberrant right subclavian artery and vascular ring. Serum calcium and parathyroid hormone levels were within normal range. No abnormalities were noted on renal ultrasound. The baby remains clinically well and will have ongoing follow-up in the Immunology and 22q clinics at McMaster Children’s Hospital.
Figure 1:
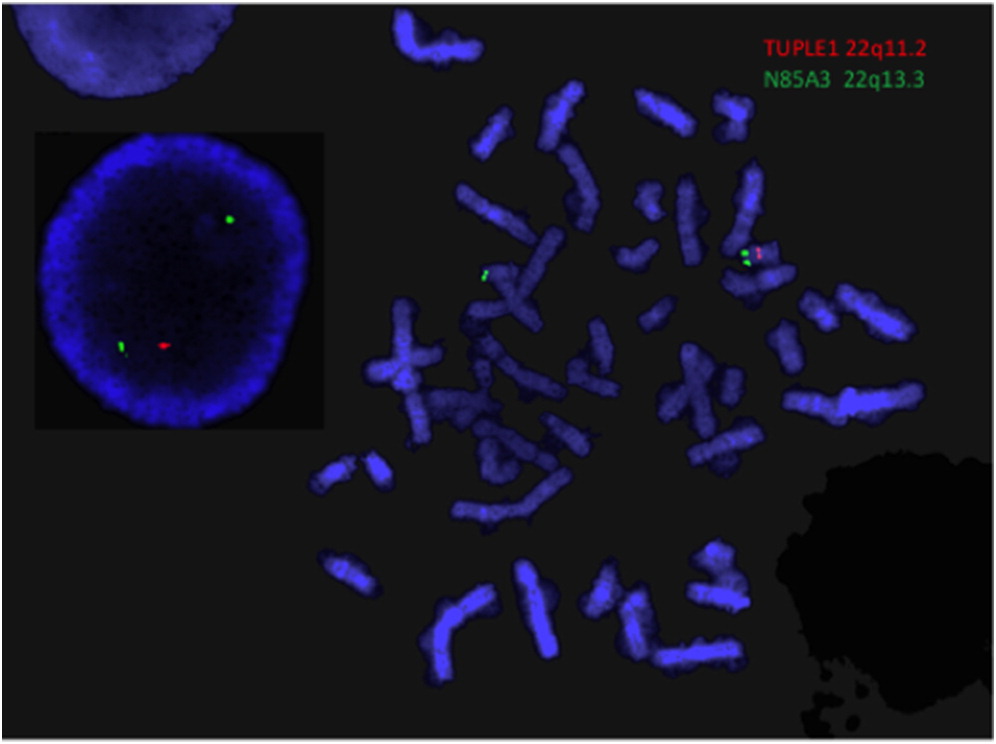
Figure 2:
Discussion
Technical details of NBS TBX1 analysis
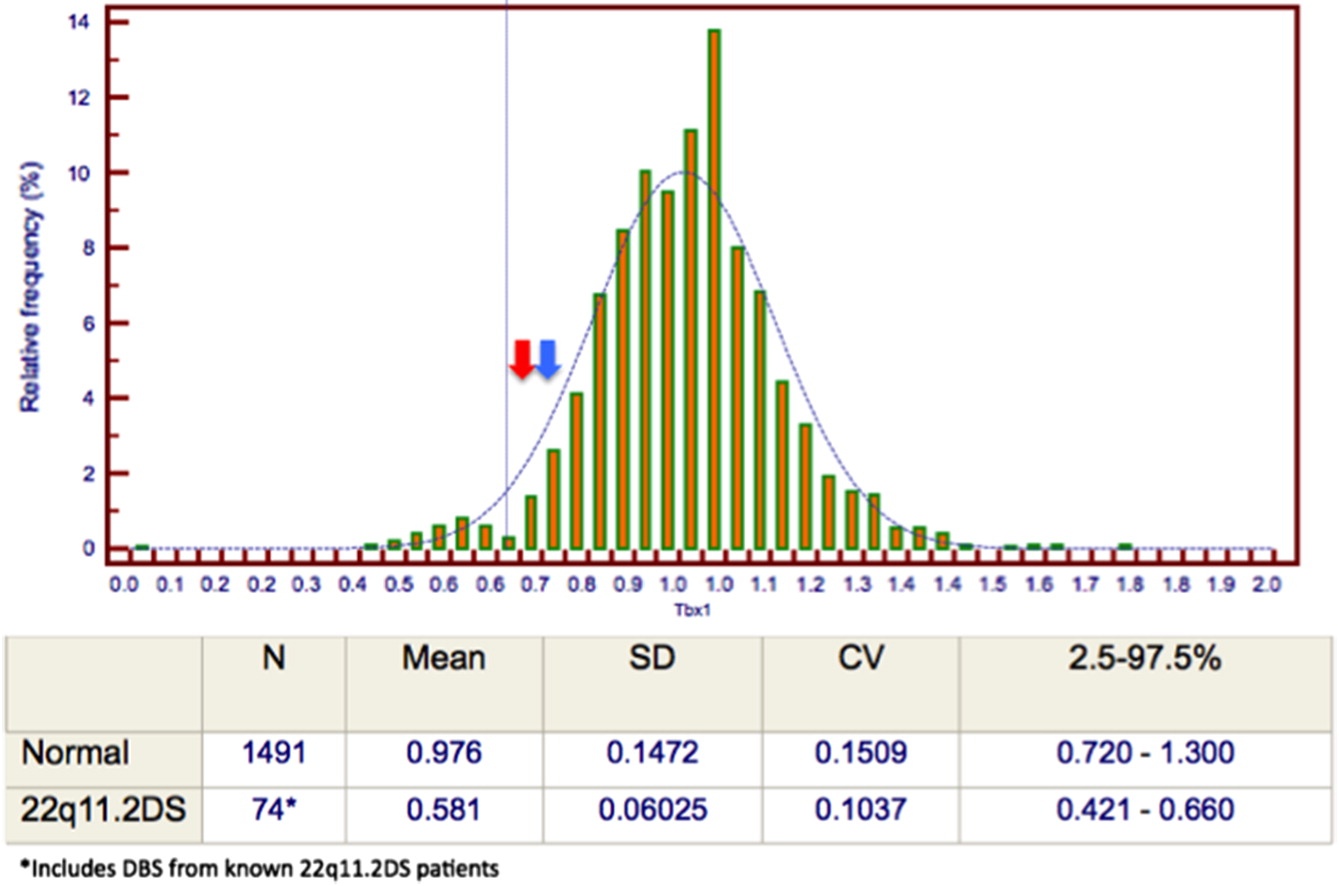
In the SCID NBS, TBX1 analysis uses PCR quantification of DNA that relies on a threshold cutoff, rather than a specific probe, as used in FISH, to screen for deletions. A ratio of patient sample (index case) to expected (control) TBX1 material is generated, with a normal ratio of 1 (range 0.75–1.25) indicating no deletion detected, and a ratio of 0.5 (range 0.25–0.75) suggestive of a deletion. The specific cutoff values were generated from data from known patients with 22q11.2DS. The set cutoff for a deletion to produce a positive screen was 0.62 at the time that our patient’s sample was processed (Figure 3). Our patient’s initial screening sample and follow-up sample ratios were 0.72 and 0.63, respectively. Both of these values fell above the cutoff that was used at the time to identify a deletion and positive TBX1 screen; thus, our patient’s deletion was not identified based on this screening method. Based on data fed back to the NBS centre through NBS follow-up protocol, the cutoff value has since been increased to a ratio of 0.66.
Figure 3:
Conclusion
This case of 22q11.2DS with a typical deletion encompassing the TBX1 gene not identified by initial TBX1 screening highlights the limitations of this test as a standalone screening assay. To our knowledge, this is the first such case to be described in the literature. As the diagnosis of 22q11.2DS has broad implications for further investigation, management and counselling, we propose that diagnostic testing with FISH and (or) CMA for 22q11.2DS is required after a NBS demonstrating low TRECs, regardless of the result of the TBX1 screening analysis.
As routine screening for SCID in Canada only began in 2013, data regarding process and outcomes remain limited. The described case demonstrates a need for a standardized follow-up testing algorithm across Canadian institutions for newborns who screen positive for SCID, which should include definitive diagnostic testing for 22q11.2DS. Further study will help to determine a comprehensive protocol to follow a low TREC result.
REFERENCES
Dorsey M. and Puck J. 2017. Newborn screening for severe combined immunodeficiency in the US: Current status and approach to management. Int. J. Neonatal Screen. 3(2):15.
Kwan A. and Puck J. 2015. History and current status of newborn screening for severe combined immunodeficiency. Semin. Perinatol. 39(3):194–205.
McDonald-McGinn, D.M., Emanuel, B.S., and Zackai, E.H. 2013. 22q11.2 deletion syndrome [online]. GeneReviews. Available from https://www.ncbi.nlm.nih.gov/books/NBK1523/ [accessed 15 July 2017].
McDonald-McGinn D.M., Sullivan K.E., Marino B., Philip N., Swillen A., Vorstman J.A., Zackai E.H., Emanuel B.S., Vermeesch J.R., Morrow B.E., Scambler P.J., and Bassett A.S. 2015. 22q11.2 deletion syndrome. Nat. Rev. Dis. Primers. 1:15071.
Pretto D., Maar D., Yrigollen C.M., Regan J., and Tassone F. 2015. Screening newborn blood spots for 22q11.2 deletion syndrome using multiplex droplet digital PCR. Clin. Chem. 61(1):182–190.
Information & Authors
Information
Published In

LymphoSign Journal
Volume 5 • Number 1 • March 2018
Pages: 17 - 20
History
Received: 20 August 2017
Accepted: 2 October 2017
Accepted manuscript online: 7 November 2017
Copyright
© 2018.
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
AmandaCiccolini, LaurenBrick, ElizabethMcCready, Dennis E.Bulman, and RaeBrager. 2018. Case of 22q11.2 deletion syndrome not identified by TBX1 screening with a positive SCID newborn screen. LymphoSign Journal.
5(1): 17-20. https://doi.org/10.14785/lymphosign-2017-0009
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
