Home gammaglobulin therapy: a patient survey of intravenous and subcutaneous options in Canada
Abstract
Introduction: For close to half a century immunoglobulin replacement therapy has been the main therapy for patients unable to produce functioning antibodies. To date, both subcutaneous (SC) and intravenous delivery methods have been successful at effectively and safely replacing immunoglobulin. Home intravenous and SC therapy programs have been established and have gained attention, but the true motivation and frequency of switching from traditional hospital-based treatment to these alternatives remains unknown. This study aims to determine the willingness of patients in Canada to switch to a home-based gammaglobulin treatment program by quantifying related experiences and preferences.
Methods: A cohort of 169 patients in Ontario currently on hospital-based intravenous immunoglobulin (IVIG) replacement therapy (referral centers or community hospitals) were sent a 2.5 page survey consisting of 25 questions. Data were collected and statistically analyzed using Fisher, χ2, and McNemar tests, where P < 0.05 was considered statistically significant.
Results: Ninety-one patients responded and most agreed to consider home therapy regardless of the administration route, based on recommendations from an immunologist (IVIG, P = 0.006; SC, P < 0.001). Patients preferred switching to home IVIG rather than to SC (P = 0.01), but their concerns regarding home healthcare costs were more prominent with IVIG (P = 0.01). The main concern with current intravenous therapy was the overall loss of time (P = 0.0001), whereas for home therapy it was the loss of supervision (P = 0.0009) and possible associated costs. Patients considered home treatment more convenient, as it is less time consuming (P = 0.01), and this was perceived as an improvement in quality of life (P = 0.001). It was considered less convenient because it may be unsafe and (or) more expensive.
Conclusion: This survey demonstrates that home intravenous therapy maybe the preferred option for patients with antibody deficiency in Ontario, provided this decision was supported by a specialist in the field, secured supervision was available, and it was not associated with personal expenses.
Statement of novelty: The first study to examine patient willingness to try a new route of gammaglobulin administration at home.
Introduction
Impaired antibody production after a specific challenge occurs in primary immunodeficiencies (PIDs) that are characterized by low or undetectable levels of all immunoglobulins (Igs) (e.g., agammaglobulinemia, X-linked, or autosomal recessive), by low IgG levels (e.g., hypogammaglobulinemia, hyper-IgM syndrome, or common variable immunodeficiency), and (or) by inadequate specific antibody levels. Antibody deficiency can present early or manifest later in life and is classified by mode of inheritance and by whether the genetic defect affects T cells, B cells, or both (Cooper and Schroeder 2005). Currently, patients with these deficiencies may lead relatively healthy lives with adequate antibody replacement therapy (Cooper and Schroeder 2005).
The mainstay of therapy for antibody deficiency, regardless of the underlying cause, has been Ig replacement therapy, administered via the intravenous (IV) or subcutaneous (SC) route to reduce the frequency and severity of infections (Durandy et al. 2005).
The IV route is the most common route of administration for Ig worldwide (Hanna et al. 2003; Anderson et al. 2007) In general, intravenous immunoglobulin (IVIG) has been successfully used by many patients and is considered to be well tolerated (Cooper and Schroeder 2005; Lemieux et al. 2005). Nonetheless, in some patients there are problems associated with the IV route that can affect their care. Adverse reactions (ARs) range from mild headache and rash to rare episodes of anaphylactoid reactions (Nowak-Wegrzyn and Lederman 1999). Individual products vary in their propensity to cause ARs and the outcome can be patient specific (Schleis and Siegel 2005; MacLennan and Barbara 2006). The infusion rates and the concentrations of solutions are also factors in patients’ tolerability (Schleis and Siegel 2005). Poor venous access in some patients may result in many attempts at venipuncture for each infusion. In some patients, indwelling central venous devices are needed, with the associated risks of infection and thromboembolic complications. Most IV infusions are performed in hospitals or clinics, with increasing costs owing to hospital-based administration. However, home-based IVIG administration has been shown to be preferred by some patients and its cost was estimated to be comparable or better than SC immunoglobulin (SCIG) (Chapel et al. 2000).
The SCIG route of administration has been used in Sweden for decades (Berger 2004). The advantages of this method include a lack of need for vascular access and relative ease of self-administration when compared with self-IV infusion. Some claims have been made that self-SCIG is associated with fewer ARs, but proper studies are lacking. The disadvantages include frequent dosing because of the limited volume that can be administered at one time, slow build up of serum trough Ig levels, and patients’ reliability if self-administered at home. Lastly, the use of SCIG is contra-indicated in patients with bleeding tendencies or in those with skin conditions that affect large areas of the body surface (Helbert and Farragher 2007).
In Canada, Ig products are distributed through the Canadian Blood Services, and costs are funded through the provincial and territorial health care budgets. This has been the case for IVIG administered in hospitals, but there is no commitment to provide similar services at home. With the growing trend of “delisting” government funded services, some or all expenses of IVIG or SCIG (pump, tubing) may be downloaded onto patients and their families. In the next 10 years the United States may face similar dilemmas if the current health care system changes. Therefore, we thought that it was important to ask patients who are already in a socialized system what their preferred route of immunoglobulin administration would be.
Methods
A survey and cover letter were mailed to 169 patients (or to their parents or guardians) who were receiving gammaglobulin treatment in Ontario, Canada. All participants were known to The Hospital for Sick Children Immunology Clinic in Toronto, Ontario, and were fluent in English (99% of eligible participants). As outlined in the cover letter, completion of the survey was optional, anonymous, and participation provided implied consent to publish the results. The subjects were given 4 weeks to return the survey, and follow-up was done with a second reminder mailing. All study responses were returned via prepaid Canada Post envelopes. The surveyed population included both children and adult patients, ranging in age from 2 to 75 years. Diagnoses included X-linked and congenital agammaglobulinemia, CD40 ligand deficency, Common Variable Immunodeficiency (CVID), selective antibody deficiency, and genetic syndromes with associated antibody deficiency.
The survey consisted of 25 questions. Eleven questions dealt with demographics, current treatment, and progress; 4 queries were on IVIG and SC (including an optional ranking for each); followed by 2 ranking questions on convenience, and 8 yes or no answers on treatment decision making. These questions encompassed patients’ experiences with current gammaglobulin treatment, what considerations would be important to them before switching to another route of administration (i.e., SC gammaglobulin treatment), and their preference for treatment at home versus hospital. The survey was reviewed by independent research experts with experience in developing surveys and our internal Research Ethics Review Board.
All anonymous survey responses were collected into a database and analyzed by a researcher unknown to the patients. Statistical analysis was performed using Analyze-it Standard (Analyze-it Software Ltd. Leeds, U.K.) for Microsoft Excel. Fisher, χ2, and McNemar tests were performed as required and considered statistically significant when P < 0.05. All results are the mean ± SD or percentages.
Qualitative and quantitative analyses of ranked questions
The rankings of the optional questions were analyzed both qualitatively and quantitatively. Qualitative analysis was conducted on all responses by adding up the total number of subjects who selected a specific option as a concern. The option that was selected the most was given the highest ranking, whereas the option selected the least was given the lowest ranking. Quantitative analysis was performed by grouping all of the subjects who ranked the options and averaging out the ranked selections. P values were then calculated for both sets of data as described.
Results
Demographics
A total of 91 patients participated in the survey (55 male, 35 female, 1 unknown) for a 54% response rate. The mean subject age was 23 ± 15 years and the mean number of years on IVIG therapy was 13.3 ± 8.5 years. Of the 91 surveys returned, 39 were completed by the parents or guardians of the patients, 41 by the patients, and 5 by both (Table 1). Seventy patients were 34 years or younger and 16 were 35 years or older. All patients had evidence for low serum IgG levels and (or) abnormal antibody response to vaccinations before IVIG replacement was initiated. Eighty-two patients received IVIG on a 28 ± 3 day interval, whereas 8 were on a 21 ± 3 day schedule. Community hospitals were the primary location of IVIG administration for 55 patients and 27 patients were routinely treated in a referral center.
Table 1:

Efficacy and safety
To assess the efficacy of current IVIG therapy, patients were asked about their perception of reduced infections as well as improved energy, concentration, and performance. An overwhelming 86% reported reduced infections since commencing IVIG therapy (P < 0.001); and 45% (P = 0.001), 16% (P = 0.131), and 12% (P = 0.012) similarly expressed improved energy, concentration, and performance, respectively. To address the safety of the current therapy regimen, patients were asked to select the frequency (always, sometimes, rarely, or never) of experiencing the 4 most common ARs associated with IVIG; headaches, fever, hives, and chills. The majority of patients did not experience any of the common ARs (P < 0.001 for fever, hives, and chills). Some patients reported having headaches always to rarely (P = 0.01). In addition, nausea and fatigue were reported by 3 patients. These results suggest that ARs for current IVIG regimens are rarely experienced.
Intravenous treatment in a hospital setting
To account for patient dissatisfaction with current IVIG therapy, subjects were asked to select the most unpleasant experiences related to IVIG therapy. They were given 6 choices and requested to select all that apply. An option to rank their selections was provided with 1 being most unpleasant and 6 being the least unpleasant. Qualitative ranking was calculated for all answers and quantitative ranking was only calculated for the subjects who ranked their choices. Lost time and the infusions themselves were listed as major concerns (ranked first and second, respectively), whereas the hospital registration process was the least important issue (ranked sixth) (Table 2). Travel time ranked fourth. Qualitative and quantitative analysis of this data could not consistently rank a placement for waiting time and adverse events (Table 2). Waiting time as a concern placed third in the qualitative analysis and fifth quantitatively out of six options. Adverse reactions showed reversed results ranking fifth for the qualitative analysis and third for the quantitative analysis. When analyzing data according to age, patients under 35 years were significantly more concerned with time (waiting time and lost time) than patients 35 years and older (P = 0.05 and 0.029, respectively, Table 3). Similarly, waiting time was significantly more important to parents rather than to patients (P = 0.038). When analysis was performed according to location of treatment, 53% of patients receiving IVIG in the community were more concerned with ARs when compared with the 22% of referral center based patients (P = 0.009).
Table 2:

Table 3:
Patients were asked which strategy they would adopt if home IVIG became available. Only 64% of all patients agreed that they would switch from hospital- to home-based treatment, but only after consulting with their immunologist (P = 0.006, Figure 1). The majority of patients said they would not switch to home from hospital treatment based on a recommendation from their family physician (P < 0.001), if a nurse was present (P < 0.001), if a family member was trained to perform venipuncture (P < 0.001), even after home therapy was proven successfully in Canada (P = 0.0007), or they would switch right away without hesitation (P < 0.001). Possible costs associated with home therapy were also not listed as a reason to change from hospital to home; however, this was not statistically significant (Figure 1). By examining age subpopulations, the costs associated with home therapy stand out as one of the major concerns for patients 35 years and older and those receiving therapy in the community (P = 0.017 and 0.049, respectively, Figure 1). A similar trend was seen when patient concerns about cost were compared with parents; but this was not statistically significant (Figure 1). Interestingly, patients 35 years and older favored home IVIG if a nurse was present to assist them (P = 0.03). In addition, although all patients agreed that training of a family member in IVIG administration would not be essential to change to home therapy, significantly fewer patients over 34 years of age agreed with this (P = 0.046, Figure 1).
Figure 1:

Subcutaneous treatment
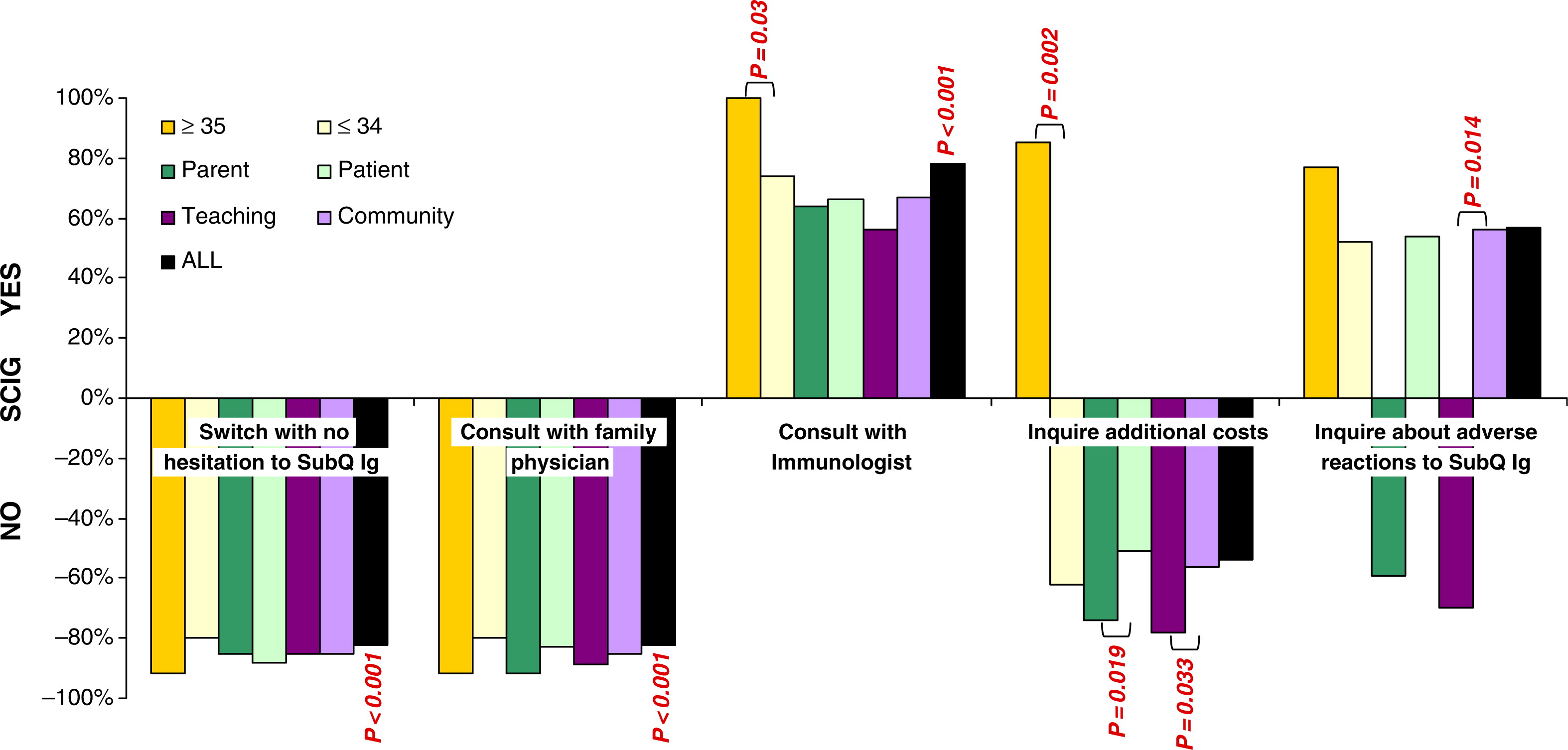
Analogous to the IVIG question, patients were asked if SCIG treatment was available and was equally effective as IVIG, which strategy they would adopt in switching to SCIG. Similar to the IVIG answers, 78% of all patients would switch to SCIG after consulting with their immunologist (P < 0.001, Figure 2). Although not significant statistically, 57% of patients agreed to switch to SCIG after inquiring about ARs. Patients would not switch from hospital to home SCIG therapy based on a consultation with their family physician (P < 0.001) or consider switching right away without hesitation (P < 0.001). Expenses associated with home SCIG therapy was less of a concern, but this was not statistically significant (Figure 2). When the surveys were reviewed according to age subgroups, costs were found to be an important issue. Patients 35 years of age and older would switch to SCIG only after inquiring about costs (P = 0.002, Figure 2) in contrast with patients under 35 years of age who were not concerned about costs. Patients receiving treatment in the community were significantly more concerned with costs of SCIG when compared with those receiving therapy at a referral facility (P = 0.033). Similarly, patients who completed the survey were significantly more concerned about costs of SCIG versus parents who completed the survey (P = 0.019). In both cases, these cost concerns were not great enough to deter switching to SCIG because the majority of respondents answered no to this question.
Figure 2:
Patients were then asked about their concerns regarding home SCIG. They were given 6 options and asked to choose all that apply, with an option to rank their choices, where 1 is most important and 6 is least important (Table 4). All responses were qualitatively ranked and subjects who decided to rank their selections were quantitatively ranked as well. Loss of supervision was ranked as the primary concern for both the quantitative and qualitative analysis. Loss of time, poking themselves, and supply storage were consistently ranked fourth, fifth, and sixth, respectively. A uniform ranking was not determined for the qualitative and quantitative analysis of costs and frequent injections. Qualitative investigation placed costs as second out of 6, whereas quantitatively it ranked as third out of 6 (Table 4). Frequent injections ranked third for the qualitative analysis and second for the quantitative analysis. This discrepancy is possibly explained when dissecting the surveys according to demographic clusters. The number one concern of patients 35 years of age and older, patients receiving community based therapy, and patients who completed the survey themselves was costs (P = 0.02, 0.038, and 0.005, respectively) when compared with patients 34 years of age and younger, patients receiving therapy in a teaching hospital, and parents who completed the survey (Figure 3). In addition, patients receiving community-based treatment were more concerned about time lost (P = 0.049, ranked third) and poking themselves (P = 0.037, ranked fourth) versus patients receiving treatment in teaching hospitals (ranked fourth and fifth, respectively, not shown).
Figure 3:
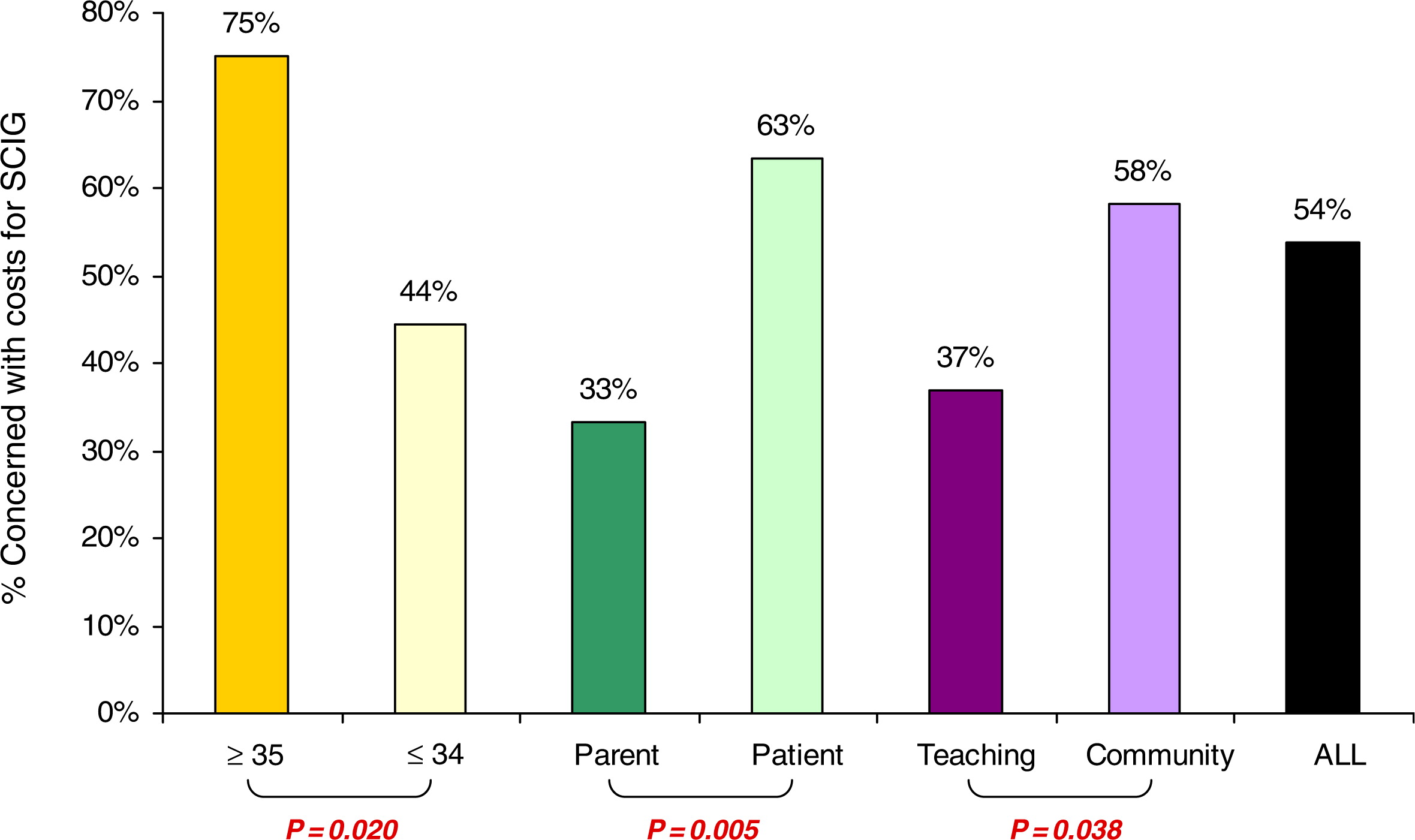
Table 4:
IVIG versus SCIG
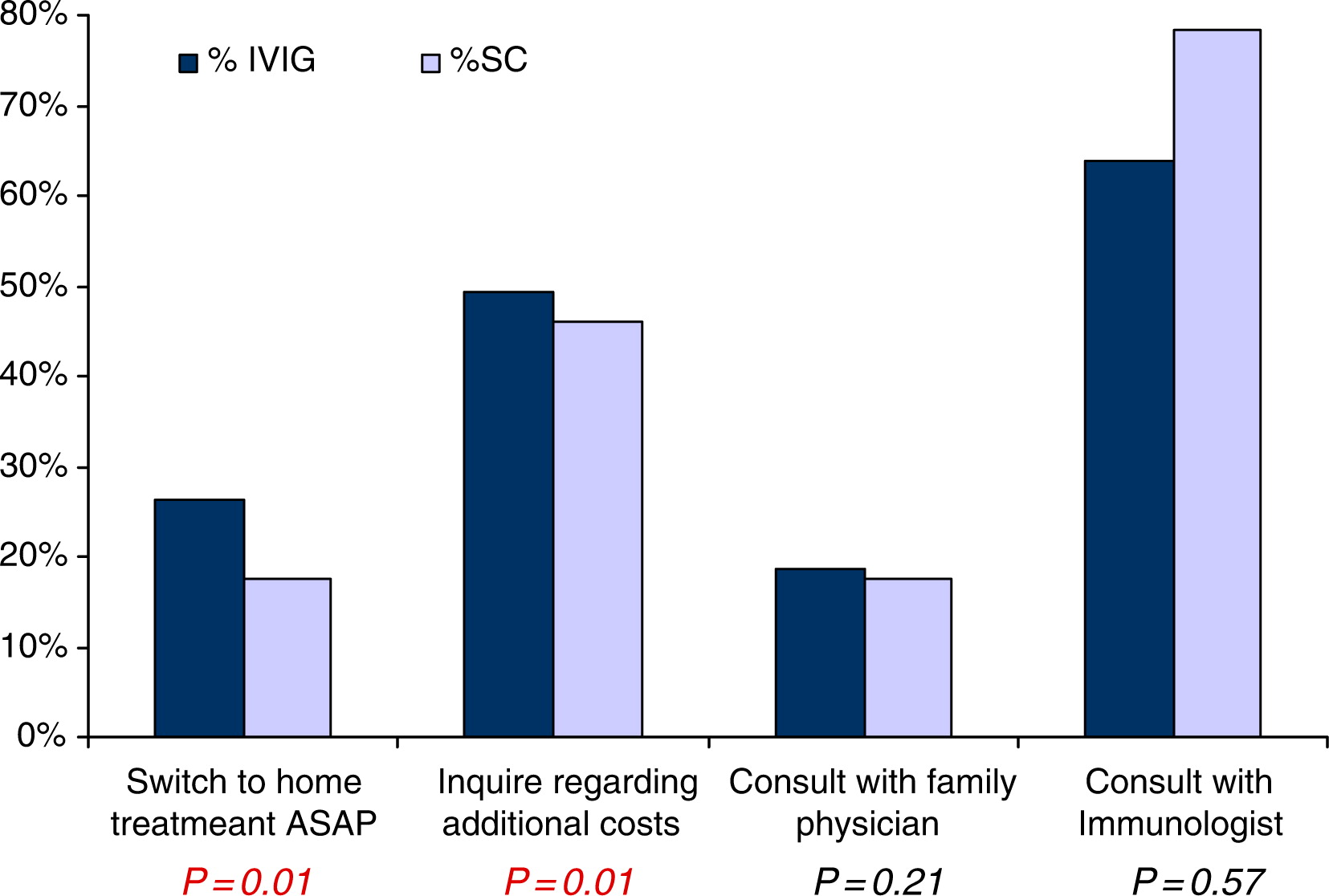
Using McNemar tests we compared the results of the IVIG answers with the SCIG answers (Figure 4). Interestingly patients were significantly more likely to switch to home IVIG rather than home SCIG (P = 0.01), but they had significant concerns regarding costs with home IVIG rather than home SCIG (P = 0.01). No significant differences were seen between consultation with their immunologist or family physician.
Figure 4:
Home treatment
Patients were then asked to rank 5 options as to why home treatment would be more convenient than hospital-based therapy (Table 5). A rank of 1 was considered most important and a ranking of 5 was considered least important. Elimination of travel time was listed at the most convenient option (P = 0.01) by all patients, followed by nicer at home (P = 0.003), better quality of life (P = 0.001), and lastly, reduced travel costs (P = 0.01). Safer at home was ranked third but was not statistically significant (P = 0.689). When the surveys were reviewed in subgroups additional trends were noted. Patients from tertiary centers ranked safety at home as the most important option related to home treatment when compared with patients receiving treatment at a community facility (Table 5). This may explain why home safety was not found to have a statistically significant distribution. In addition, patients 35 years of age and older ranked travel time in fourth place instead of first place, as ranked by the patients under 35 years of age (Table 5).
Table 5:
To better understand why certain patients might not want to switch to home therapy, 5 possibilities signifying the inappropriateness of home therapy were ranked by patients with a ranking of 1 being most inappropriate and 5 being the least inappropriate. When analyzing the data for all patients, an overall ranking could not be determined. However, the data illustrated that patients under 35 years of age, parents who completed the survey, and patients receiving treatment at a teaching hospital all agreed that home therapy was primarily unsafe (Table 6). Their second major concern was having fewer doctor visits, whereas cost appeared to be of little concern as it was ranked last. Interestingly, we found the opposite for patients 35 years of age and older, patients who completed the survey, and community-based patients. They listed associated costs as their number one concern and lack of safety and fewer doctor visits as the least of their concerns. The ranking of responsibility for supplies and more work for guardian or spouses varied across all groups.
Table 6:

Treatment decisions
The final group of queries was a set of 8 yes or no answers to patient treatment responsibilities if home therapy were to become available. Table 7 illustrates the answer to each question and the associated P value. Of particular note is that patients were not comfortable taking responsibility for their infusions (P = 0.032). Patients also preferred IVIG infusions over SCIG infusions because they take less time (P = 0.005) and patients did not believe that SCIG infusions 2 times per week are less traumatic than IVIG once per month (P = 0.003). A nurse being present did not have any significantly influence whether a patient would switch to home therapy.
Table 7:
Discussion
Safety and efficacy
IVIG has been previously shown to be effective in reducing infections and improving outcomes for lung disease (Roifman et al. 1987; Chapel et al. 2000; Bhole et al. 2008). In this survey, patients confirmed they have had a decrease in the frequency of infections as well as improved energy, concentration, and performance.
Headaches are the most common AR known to be associated with immunoglobulin treatment followed by fever, chills, and hives (Peirce et al. 2003; Ochs et al. 2006). In this survey the frequency of these commonly reported ARs appear to be rare. This may be attributed to the referral center practice of managing reactions by maintaining patients on a consistent IVIG product brand; instructing patients to be well hydrated pre-, during, and post-infusion; the use of pre-medications if required; and managing infusion rates to the highest tolerated rate (Peirce et al. 2003; Ochs et al. 2006). Despite this finding, our patient population appeared to still have concerns regarding potential ARs. Patients infused in community hospitals ranked ARs as a major concern with their current IVIG treatment (Table 3) or with putative switching to SC treatment (Figure 2). This finding may reflect less vigilance in adjusting infusion practices and monitoring of post-infusion ARs in community hospital settings. An interesting finding was that home treatment was perceived as unsafe among patients receiving therapy in teaching hospitals, parents of IVIG treated children, and patients under 35 years of age (Table 6). This conservative view may change over time once a credible home-based treatment system wins the confidence of patients.
Costs
Costs are an underlying factor in the implementation of a home based immunoglobulin treatment program. Under the Canadian Health Act (1985), hospital and physician care is a universal entitlement (Canadian Home Care Association, 2008). However, home healthcare does not have any minimal claim under this legislation. As a result, the majority of funding today for the home healthcare sector comes from private support, as provinces can pick and choose which programs are eligible and the amount they will cover (Peter et al. 2007). Since the early 1990s, the number of Canadian home healthcare patients have increased, whereas average provincial spending has decreased (Williams et al. 2005; Peter et al. 2007; Canadian Home Care Association 2008). With this current system it is no surprise that patients ranked costs as the second or third most important concern regarding home therapy (Table 4) and that the most concerned patients werethose 35 years of age and older and those receiving their therapy in the community (Figures 1 and 3). Many reports out of Europe and the United States have indicated a cost savings or at least a break-even budget for a self-infusion system (Ochs et al. 1987; Sorensen et al. 1987; Ryan et al. 1988; Gardulf et al. 1995b; Kobayashi et al. 1990; Gaspar et al. 1998; Högy et al. 2005; Membe et al. 2008). A recent Canadian cost assessment comparing home- to hospital-based treatment revealed some marginal cost savings for home-based IVIG or SCIG replacement (Membe et al. 2008). However, it remains uncertain whether costs for home-based treatment will be fully recovered from the government-owned insurer.
Quality of life
The possibility of an improved quality of life is one of the motivators for a home-based self-infusion program for patients with antibody deficiencies. Quality of life is recognized as the patient's perception of the impact of disease and treatment on daily life. Previous studies have demonstrated an improved quality of life because of decreased time loss from school or work, lower costs, greater independence, better knowledge of their condition, fewer interruptions with daily activities, increased self-confidence, and better disease management (Sorensen et al. 1897; Ochs et al. 1986; Sigstad et al. 2005; Bhole et al. 2008). Surprisingly, patients in our study ranked quality of life as second last in terms of convenience for home therapy (Table 5). However, they also believed it would be nicer to be treated at home and they preferred to eliminate travel to the hospital.
Preferences
A limited number of small and uncontrolled clinical trials have been conducted suggesting a patient preference for home therapy (Gardulf et al. 1995a; Abrahamsen et al. 1996; Hansen et al. 2002; Gardulf et al. 2004; Bhole et al. 2008). In fact, SCIG has only been widely used in Sweden, a country that traditionally did not use IVIG (Berger 2004). These trials, however, never measured a population's willingness to switch, only its preference after commitment. This is the first reported survey determining whether this is an acceptable option for the patient population prior to the initiation of a clinical trial. Patients in our cohort were open to the idea of learning how to inject SC or IVIG, but they disagreed that home-based treatment is always better than hospital-based treatment. If switching to home treatment, this survey suggested that patients would prefer IVIG once per month over more frequent SC injections.
The majority of the patients surveyed agreed they would switch after consulting with an immunologist regardless of therapy type (Figures 1 and 2). Because almost half of the survey participants were treated in 1 tertiary care center, factors such as the complexity of cases and the model of practice could have influenced the responses. Indeed, many of the patients treated in the tertiary referral center have either associated comorbidities or chronic complications of their PID. Further, the model of practice that allows unrestricted access to an advanced practice nurse, fellows training in immunology, and staff immunologists for healthcare concerns regarding management of their disease may have influenced this finding. Nevertheless, immunologists should be aware of this perception by patients and should act responsibly when making treatment suggestions to patients.
In addition, we found loss of time was the number one concern with the current regimen (Tables 2 and 5), supporting the notion of convenience of treatment at home. Interestingly, when patients were divided into age groups under and over 35 years of age, lost time was more of a concern for the younger age group. This finding suggests that patients may require different models of care at different times in their lives. As this treatment is required for life, replacement gammaglobulin programs should allow for flexibility of route of administration and for the place of replacement therapy to reflect patients’ changing lifestyle needs.
It has been previously suggested that patients may prefer SCIG treatment (Nicolay et al. 2006; Bhole et al. 2008). Contrarily, our study shows that the 91 IVIG patients surveyed are more likely to switch to home IVIG rather than to SC (Figure 4). This preference for home IVIG may stem from the frequency and trauma of SCIG injections (Tables 4 and 7) (Gardulf et al. 1995a; Abrahamsen et al. 1996; Hansen et al. 2002).
The inability of patients to accurately rank the inappropriateness of home therapy (Table 6) suggests patients may favor this option. However, concerns associated with switching to home treatment remained. The primary concerns reported by patients were loss of medical supervision and responsibility for their own treatment (Tables 4 and 7). This may reflect patients’ anxiety over fewer doctor visits (Table 6, ranked second for inappropriateness) for patients under 35 years of age as well as for parents and patients at teaching hospitals. Some of these concerns may be alleviated by robust training and education of patients, association to an infusion center, and access to national patient PID organizations (Asthida and Saxon 1986; Ochs et al. 1986; Ochs et al. 1987; Sorensen et al. 1987; Chapel et al. 1988; Kobayashi et al. 1990; Brennan et al. 1995; Sigstad et al. 2005; Bhole et al. 2008).
Conclusions
Although patients find their current treatment effective at managing their antibody disorder with few to no ARs, there may be support for a home-based gammaglobulin therapy program for Canadian patients. This transition, however, is based on approval by immunologists. A statistically significant preference for an intravenous program was illustrated in comparison with a subcutaneous home protocol. The loss of time and travel-associated costs with hospital-based programs could be alleviated through a home-based treatment plan if funding is established to cover the gammaglobulin product.
Acknowledgement
The work was supported by the Canadian Center for Primary Immunodeficiency, The JMF Research Laboratories for the diagnosis of Primary Immunodeficiencies, and by a grant from Immunodeficiency Canada.
REFERENCES
Abrahamsen T.G., Sandersen H., and Bustnes A. Home therapy with subcutaneous immunoglobulin infusions in children with congenital immunodeficiencies Pediatrics. 1996 98 1127 -1131
Anderson D., Ali K., Blanchette V., Brouwers M., Couban S., and Radmoor P. Guidelines on the use of intravenous immune globulin for hematologic conditions Transfus. Med. Rev. 2007 21 S9 -S56
Asthida E.R. and Saxon A. Home intravenous immunoglobulin therapy by self-administration J. Clin. Immunol. 1986 6 306 -309
Berger M. Subcutaneous immunoglobulin replacement in primary immunodeficiencies Clin. Immunol. 2004 112 1 1 -7
Bhole, M.V., Burton, J., and Chapel, H.M. 2008. Self-infusions programmes for immunoglobulin replacement at home: feasibility, safety and efficacy. In Immunology and Allergy Clinics of North America. Roifman Cm Alam R. Philadelphia. WB Saunders Company. pp. 821–832.
Brennan V.M., Cochrane S., Fletcher C., Hendy D., and Powell P. Surveillance of adverse reactions in patients self-infusing intravenous immunoglobulin at home J. Clin. Immunol. 1995 15 116 -119
Canadian Health Act. 1985. C.6, s.1.
Canadian Home Care Association. 2008. Portraits of home care: a picture of progress and innovation. Ottawa, ON. Available at www.cdnhomecare.ca.
Chapel H., Brennan V., and Delson E. Immunoglobulin replacement therapy by self-infusion at home Clin. Exp. Immunol. 1988 73 160 -162
Chapel H.M., Spickett G.P., Ericson D., Engl W., Eibl M., and Bjorkander J. The comparison of the efficacy and safety of intravenous verses subcutaneous immunoglobulin replacement therapy J. Clin. Immunol. 2000 20 94 -100
Cooper, M.D., and Schroeder, H.W. 2005. Primary immune deficiency diseases. In Harrison's principles of internal medicine. 16th ed. Edited by Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser S, Jameson JL. McGraw-Hill, New York. pp. 1939–1947.
Durandy A., Wahn V., Petteway S., and Gelfand E.W. Immunoglobulin replacement therapy in primary antibody deficiency diseases - maximizing success Int. Arc. Allerg. Immunol. 2005 136 3 217 -229
Gardulf A., Bjorvell H., Anderson V., Bjorkander J., Ericson D., Froland S.S., Gustafson R., Hammarstrom L., Nystrom T., Soeberg B., and Smeith C.I.E. Lifelong treatment with gammaglobulin for primary antibody deficiencies: the patients' experiences of subcutaneous self-infusions and home therapy J. Advan. Nur. 1995 21 917 -927
Gardulf A., Hammarstrom L., Gustafson R., Nystrom T., Smith C.I.E., Jonsson E., Moller G., Ericson D., Soeberg C., Froland S., Jacobsen M.B., Anderson V., and Bjorkander J. Subcutaneous immunoglobulin replacement in patients with primary antibody deficiencies: safety and costs Lancet. 1995 345 365 -369
Gardulf A., Nicolay U., Asensio O., Bernatowska E., Bock A., Costa-Carvalho B., Granert C., Haag S., Hernandez D., Kiessling P., Kus J., Matamoros N., Niehues T., Schmidt S., Schulze I., and Borte M. Children and adults with primary antibody deficiencies gain quality of life by subcutaneous IgG self-infusions at home J. Allerg. Clin. Immunol. 2004 114 936 -942
Gaspar J., Gerritsen B., and Jones A. Immunoglobulin replacement treatment by rapid subcutaneous infusion Arc. Dis. Child. 1998 79 48 -51
Hanna K., Poulin-Costello M., Preston M., and Maresky N. Intravenous immune globulin use in Canada Can. J. Clin. Pharmacol. 2003 210 1 11 -16
Hansen S., Gustafson R., Smith C.I.E., and Gardulf A. Subcutaneous IgG infusions in patients with primary antibody deficiencies: decreased time of delivery with maintained safety Clin. Immunol. 2002 104 237 -241
Helbert M. and Farragher A. Subcutaneous immunoglobulin for patients with antibody deficiency Hosp. Med. (London). 2007 68 4 206 -210
Hogy B., Keinecke H.O., and Borte M. Pharmacoeconomic evaluation of immunoglobulin treatment in patients with antibody deficiencies from the perspective of the German statutory health insurance Europ. J. Health. Econ. 2005 6 24 -29
Kobayashi R.H., Kobayashi A.D., Lee N., Fischer S., and Ochs H.D. Home self-administration of intravenous immunoglobulin therapy in children Pediatrics. 1990 85 705 -709
Lemieux R., Bazin R., and Néron S. Therapeutic intravenous immunoglobulins Mol. Immunolog. 2005 42 7 839 -848
MacLennan S. and Barbara J.A.J. Risks and side effects of therapy with plasma and plasma fractions Baill. Best Pract. Res. Clin. Haematolog. 2006 19 1 169 -189
Membe, S.K., Ho, C., Cimon, K., Morrison, A., Kanani, A., and Roifman, C.M. 2008. Economic assessment of different modalities of immunoglobulin replacement therapy. In Immunology and Allergy Clinics of North America. Roifman CM Alam R. Philadelphia. WB Saunders Company. pp. 861–874.
Nicolay U., Kiessling P., Berger M., Gupta S., Yel L., Roifman C.M., Gardulf A., Eichmann F., Haag S., Massion C., and Ochs H.D. Health related quality of life and treatment satisfaction in North American patients with primary immunodeficiency diseases receiving subcutaneous gammaglobulin infusions at home J. Clin. Immunol. 2006 26 1 65 -72
Nowak-Wegrzyn A. and Lederman H.M. Supply, use, and abuse of intravenous immunoglobulin Cur. Opin. Pediat. 1999 11 6 533 -539
Ochs H.D., Fischer S.H., and Lee M.L. Intravenous immunoglobulin home treatment for patients with primary immunodeficiency diseases Lancet. 1986 1 610 -611
Ochs H.D., Gupta S., Kiessling P., Nicolay U., and Berger M. Safety and efficacy of self-administered subcutaneous immunoglobulin in patients with primary immunodeficiency diseases J. Clin. Immunol. 2006 26 265 -273
Ochs H.D., Lee M.L., Fisher S.H., Delson E.S., Change B.S., and Wedgwood R.J. Self-infusion of intravenous immunoglobulin by immunodeficient patients at home J. Infect. Dis. 1987 156 652 -654
Peirce L.R. and Jain N. Risks associated with the use of intravenous immunoglobulin Transfus. Med. Rev. 2003 17 241 -251
Peter E., Spalding K., Kenny N., Conrad P., McKeever P., and Macfarlane A. Neither seen nor heard: children and homecare policy in Canada Soc. Sci. Med. 2007 64 1624 -1635
Roifman C.M., Levison H., and Gefland E.W. High-dose verses low-dose intravenous immunoglobulin in hypogammaglobulinemia and chronic lung disease Lancet. 1987 1 1075 -1077
Ryan A., Thomson B.J., and Webster A.D. Home intravenous immunoglobulin therapy for patients with primary hypogammaglobulinemia Lancet. 1988 2 79
Schleis, T., and Siegel, J. 2005. Formulary considerations for IGIV products. U.S. Pharmacist, East Rutherford, NJ. ACPE Program No 430-000-05-021-H01.
Sigstad H.M., Stray Pedersen A., and Froland S.S. Coping, quality of life, and hope in adults with primary antibody deficiencies Health. Qual. Life. Outcomes. 2005 3 31
Sorensen R.U., Kallick M.D., and Berger M. Home treatment of antibody-deficiency syndromes with intravenous immune globulin J. Allerg. Clin. Immunol. 1987 80 810 -8155
Williams, P.A., Spalding, S., Deber, R.B., and McKeever, P. 2005. Prescriptions for pediatric home care: analyzing the impact of the shift from hospital to home and community on children and families. SickKids Foundation, Toronto, ON.
Information & Authors
Information
Published In
LymphoSign Journal
Volume 01 • Number 01 • September 2014
Pages: 27 - 37
History
Received: 8 April 2014
Accepted: 9 April 2014
Accepted manuscript online: 16 June 2014
Version of record online: 16 June 2014
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
ReidBrenda and PiresLinda. 2014. Home gammaglobulin therapy: a patient survey of intravenous and subcutaneous options in Canada. LymphoSign Journal.
01(01): 27-37. https://doi.org/10.14785/lpsn-2014-0001
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
