Precision medicine applications for severe asthma
Abstract
Asthma is a heterogeneous condition in which multiple pathological pathways manifest with similar symptoms. Severe asthma (SA) is challenging to manage and comprises a significant health and economic burden. Many studies have been conducted in an attempt to define different clinical phenotypes that translate into biological endotypes, with the goal of tailoring treatment based on precision medicine. This review summarizes the current evidence for the treatments of SA, and in particular, the biologic treatments that are currently available: omalizumab, mepolizumab, reslizumab, benralizumab and dupilumab. We found only limited high-quality direct evidence regarding treatment with anti-IgE (omalizumab) in SA patients. Data regarding anti-interleukin (IL)-5 (mepolizumab, reslizumab and benralizumab) showed beneficial effects in severe eosinophilic asthma (SEA) with different levels of blood eosinophils used in clinical trials. Dupilumab, anti-IL-4/IL-13, was shown to be effective in SEA and is the only agent currently FDA-approved for the indication of oral corticosteroid dependent asthma, regardless of the blood eosinophil level. This review also summarizes the existing knowledge regarding the characteristics of the patient who may respond to the different therapies. As of today, more studies are needed to better understand the diverse mechanisms that underlie SA phenotypes. We have not yet adequately reached the goal of precision medicine. Additional studies are necessary in order to find novel surrogate markers that can predict the response to a specific biologic therapy, especially in patients who are oral corticosteroid dependent. In addition, efforts must be invested into research looking for new treatment options for patients with non-type-2 inflammation SA.
Statement of novelty: we review the current evidence regarding tailored treatment therapies in SA, with a particular focus on the knowledge regarding patient selection for specific biologic treatments.
Introduction
Asthma is a heterogeneous condition in many respects, including onset of disease, severity, inflammatory pathways and response to treatment (Busse 2019). Severe asthma (SA) is defined as asthma that is uncontrolled despite adherence with maximal optimized Global Initiative for Asthma (GINA) step 4 or step 5 therapy [high-dose inhaled corticosteroids (ICS) and long acting beta agonists (LABA) with or without leukotriene modifiers] and treatment of contributory factors. Also included is controlled asthma that worsens on tapering of this high-dose treatment (GINA 2019).
SA occurs in 3%–10% of all asthma patients and comprises a significant health burden (Chung et al. 2014; Lang 2015; GINA 2019). For the physician, SA patients may be challenging to manage. Today, with the growing recognition of phenotypic differences within this group of patients, there are several treatment options that benefit some but not all patients. Precision medicine can assist in tailoring an individual treatment plan for each patient. The ideal goal for efficient precision medicine is to define for each pharmacological treatment the patient population that is most likely to respond: based on the clinical phenotype and underlying biological endotype, without requiring excessive imaging and laboratory testing.
Most patients with asthma will respond to treatment. When a patient does not respond to treatment, questioning the diagnosis of asthma is important. Several conditions may mimic asthma (Bousquet et al. 2010). Some of these conditions share common features with asthma requiring additional tests for definitive diagnosis. These include conditions that originate in the upper respiratory system, such as vocal cord dysfunction and exercise-induced laryngeal obstruction syndrome, and illnesses that mainly involve the airways, such as tracheobronchomalacia, inhaled foreign bodies, bronchial amyloidosis and bronchiectasis. Furthermore, the differential diagnosis may also include disorders that involve both the airways and lung parenchyma, and sometimes the airway vasculature such as chronic obstructive pulmonary disease (COPD), allergic bronchopulmonary aspergillosis (ABPA) and pulmonary eosinophilic syndromes as well as other disorders such as congestive heart failure, hyperventilation syndrome (dysfunctional breathing), cystic fibrosis and obstructive sleep apnea (OSA) (Bousquet et al. 2010).
A thorough medical history and examination are of paramount importance. Additionally, chest x-ray may show signs of bronchiectasis, congestive heart failure, tumors and foreign bodies. Spirometry with reversibility can confirm the diagnosis of asthma (Carr and Kraft 2017). However, a subset of patients with SA may develop partial airway reversibility or irreversible fixed airway obstruction (Vonk et al. 2003). High-resolution computed tomography is recommended in severe asthmatics only when SA presentation is atypical, such as excessive mucus production, a rapid decline in lung function, reduced carbon monoxide transfer factor coefficient or the absence of atopy in a child with difficult asthma (Chung et al. 2014). Bronchoscopy of the upper and lower airways is relatively safe and can provide important information in a few selected patients when characterizing refractory asthma (Moore et al. 2011; Good et al. 2012).
The World Health Organization (WHO) in 2009 defined SA and classified it into 3 categories: untreated, difficult to treat, and treatment resistant (Bousquet et al. 2010). Therefore, once we confirm the diagnosis of asthma, the next step would be to differentiate between difficult to manage and treatment resistant SA. Many issues can impair asthma control in an individual patient and are thus important to assess. It is essential to review the patient’s adherence to medications and inhaler technique, and to search for factors that may exacerbate asthma, hence making it difficult to treat, such as smoking (active or passive), exposure to allergens, psychosocial issues, and comorbidities. Several comorbidities may contribute to lack of control in SA. These include allergic rhinitis and chronic rhinosinusitis, gastroesophageal reflux disease (GERD) and OSA (Carr and Kraft 2017). Once exacerbating factors have been minimized, if the patient still experiences symptoms despite the highest level of recommended therapy, they are deemed as suffering from treatment resistant SA. Also termed refractory asthma, these patients are relatively corticosteroid (CS)-insensitive. Some are only controlled with oral CS (OCS) and are referred to as steroid dependent (Bousquet et al. 2010). In this article, we will review the evidence for the current recommended treatments for SA and discuss the methods available today to better guide therapy in this group of patients.
Biomarkers in severe asthma
Several biomarkers play a role in guided therapy for patients with SA. The currently available biomarkers represent mostly type-2 (T2) inflammation and allergy. These include: blood and sputum eosinophil counts, fractional exhaled nitric oxide (FeNO) levels, periostin, immunoglobulin (Ig) E levels, skin prick tests, and specific IgE. These biomarkers play a role in treatment selection for specific biological treatments (see below). However, despite considerable research and advances, the available biomarkers do not precisely distinguish between the different phenotypes nor adequately predict treatment response (Tiotiu 2018; Kaur and Chupp 2019). T2 inflammation may be present in both allergic and non-allergic asthma (Hirose et al. 2017). We currently consider the T2 inflammatory response to be a result of a complex interaction between the innate and adaptive immunity (Fahy 2015; Aron and Akbari 2017; Sonnenberg and Hepworth 2019). T cells are the main player in the adaptive response, whereas natural killer cells and type-2 innate lymphoid cells (ILC2s) play a key role in the innate response (Aron and Akbari 2017). In response to external environmental factors (e.g., allergens, pollutants, and infectious agents), the airway epithelium releases epithelial alarmins, such as IL-25, IL-33, and thymic stromal lymphopoietin that activate downstream T cells and ILC2s (Mitchell and O’Byrne 2017). In allergic asthma, antigen stimuli induce the activity of antigen-presenting cells that promote naïve T lymphocytes to differentiate to T2 helper cells (TH2) and may also activate the ILC2s (Chen et al. 2017; Winkler et al. 2019). TH2 cells secrete several typical T2 cytokines, including IL-4, IL-5, IL-9, and IL-13 while ILC2s are effective producers of IL-5 and IL-13 but may also produce the other T2 cytokines (Hazenberg and Spits 2014; Winkler et al. 2019). In addition, IL-4 stimulates B cells and promotes class-switching and specific IgE production whereas IL-5 drives eosinophilia (Hirose et al. 2017; Kaur and Chupp 2019).
A positive skin prick test or in vitro testing for a specific IgE against at least 1 perennial clinically relevant allergen identifies sensitization and is considered a marker of allergic asthma.
Eosinophils
Initially, the term “eosinophilic asthma” referred to a sub-phenotype of asthma with elevated levels of eosinophils in the sputum (≥2%–3%, depend on the study) or bronchial biopsies despite chronic doses of ICS (De Groot et al. 2015; Price et al. 2015). In addition, studies showed that sputum eosinophil levels might predict asthma exacerbations (Veen et al. 1999; Jatakanon et al. 2000; Leuppi et al. 2001; Li et al. 2017). A recent Cochrane meta-analysis supported using sputum eosinophil counts to tailor asthma interventions in order to reduce the frequency of exacerbation in adults, and suggested there is insufficient data to support this approach in children (Petsky et al. 2017). However, sputum induction is not easy to perform. Out of all the available biomarkers, airway eosinophilia correlates best with blood eosinophilia. Therefore, blood eosinophil levels replace sputum levels both in clinical trials and in routine clinical practice (Wagener et al. 2015). Cross-sectional analysis of a Belgian registry that included 350 SA patients demonstrated a significant correlation between blood eosinophil level and sputum eosinophil count (p < 0.0001; r = 0.53) (Schleich et al. 2014). Furthermore, by using the receiver-operating characteristic (ROC) curve the author found 188 cells/mm3 to be the best cut-off of blood eosinophil level to identify a sputum eosinophil count ≥3% [Sensitivity 72.3%, specificity 72.2%, p < 0.0001, area under the curve (AUC) = 0.89]. Importantly, 53% of the participants had an eosinophil count above 220 cells/mm3, suggesting that the majority of SA patients displayed eosinophilic inflammation despite high-dose CS (Schleich et al. 2014). Data from a big UK cohort study revealed that asthma patients with eosinophil counts >400 cells/µL were more likely to have acute respiratory events and severe exacerbations (Price et al. 2015). These and other studies demonstrated the prospective for eosinophilic-targeted biologic therapies (McBrien and Menzies-Gow 2017).
Fractional exhaled nitric oxide (FeNO)
FeNO is a noninvasive measurement that is relatively easy to perform and provides information on airway inflammation. Nitric oxide synthases create nitric oxide (NO) in the airway epithelial cells. Elevated levels of NO in the exhaled breath occur during airway inflammation due to up-regulation of inducible NO synthase 2 (NOS2) by pro-inflammatory cytokines and stimuli (e.g., viruses, allergens and environmental pollutants). NOS2 expression occurs at low levels in airway epithelial cells under normal conditions and expression is glucocorticoid sensitive (Hoyte et al. 2018).
In 2011, the American Thoracic Society (ATS) published their guide on interpretation of FeNO results and proposed to characterize levels <25 parts per billion (ppb) in adults (<20 ppb in children) as low FeNO, and levels >50 ppb (>35 ppb in children) as high. They recommended interpreting levels between 25 and 50 ppb in adults with caution based on clinical presentation (Dweik et al. 2011). In the general population, there is a wide variability in FeNO levels with overlapping values between healthy individuals and asthma patients. Additionally, there are factors that affect FeNO measurements, such as smoking and use of anti-inflammatory medications which reduce FeNO levels. Atopy has been shown to increase FeNO levels. Other factors are generally less agreed upon, such as age (may be more important in children), sex, and height (results of which are less consistent). In addition to these factors, there are technical factors that may affect FeNO measurements such as technique, exhalation flow rate, and nasal NO contamination (Dweik et al. 2011).
Asthmatic patients tend to have higher levels of FeNO before starting ICS therapy while patients receiving ICS have levels similar to healthy controls (Kharitonov et al. 1994). FeNO levels correlate with airway hyper responsiveness and sputum eosinophilia (Berkman et al. 2005; Taylor 2006). In 2 independent cohorts across various severities of asthma, FeNO was a relatively good predictor for eosinophilic inflammation and it achieved the best combination of sensitivity (63%) and specificity (92%) at a rather high cut-point of 42 ppb (AUC = 0.78) (Wagener et al. 2015). Few studies showed that higher FeNO levels might assist in predicting the response to systemic steroids (Hoyte et al. 2018). Two meta-analyses, 1 in adults and 1 in children, reviewed the efficacy of tailoring asthma interventions based on FeNO in comparison to management based on clinical symptoms alone. The 2 studies reached a similar conclusion; FeNO guided therapy results in lower exacerbation rate but there was no difference between groups in other measures of asthma severity that affect day-to-day clinical symptoms or ICS dose (medications used to control asthma) (Petsky et al. 2016a, 2016b). At present, due to insufficient evidence and lack of clear benefit, neither GINA nor the ATS guidelines recommend using FeNO to guide treatment in the SA population (Chung et al. 2014; GINA 2019).
Periostin
Periostin is a matricellular protein secreted by lung fibroblasts and airway epithelium and is induced mainly by IL-13/IL-4 signaling. There is evidence that periostin is involved in subepithelial fibrosis in bronchial asthma and has a potential role in eosinophilic airway inflammation phenotypes in SA (Takayama et al. 2006; Wagener et al. 2015).
As a surrogate biomarker for T2 inflammation, periostin was used to predict the efficacy of treatments targeting IL-13 and IgE (Tajiri et al. 2016; Zissler et al. 2016). However, 2 large randomized controlled trials found inconsistent responses to anti-IL-13 in patients with high periostin levels, questioning its potential use as a predictive biomarker (Hanania et al. 2016). In children aged 6–11 years, elevated levels of periostin might mask any increase due to allergic diseases and the exact validated cut-off values for high and low serum periostin for asthma have not been determined (Inoue et al. 2015; Medrek et al. 2017; Pavord et al. 2017). Furthermore, periostin can be elevated due to other respiratory illnesses and disease states such as idiopathic pulmonary fibrosis, chronic rhinosinusitis with nasal polyposis, scleroderma, cancer and cardiovascular disease (Izuhara et al. 2016). For all these reasons, the use of periostin as a biomarker in asthma management is currently limited.
Phenotypes in severe asthma
Asthma is a heterogeneous condition in which multiple biologic pathways underlie inflammation leading to similar symptoms. Many studies have been conducted to distinguish different phenotype clusters, with the rationale that it would lead to the discovery of distinct endotypes and assist in precision medicine. Nevertheless, we still have not reached this goal because there is some heterogeneity between the phenotype clusters, the clusters show some overlap, and the methodology used and cohorts examined (Tyler and Bunyavanich 2019). A recent work by Kaur and Chupp (2019) reviews the main clustering studies, including the SA Research Program (SARP) in the United States, the Leicester study conducted in the United Kingdom, and the Unbiased Biomarkers in Prediction of Respiratory Disease Outcome (U-BIOPRED) cohort that collected data from eleven countries (Haldar et al. 2008; Moore et al. 2010; Lefaudeux et al. 2017). Cluster analysis by these 3 studies showed 4 relatively consistent clusters of patients; (i) early-onset mild allergic asthma, (ii) early-onset allergic moderate to severe remodeled asthma, (iii) late-onset non-allergic eosinophilic asthma, and (iv) late-onset non-allergic non-eosinophilic asthma (Kaur and Chupp 2019). Early-onset allergic asthma is considered to be derived from T2 cells. However, high blood eosinophil levels usually correlate with more severe allergic asthma (SAA), while in the mild form we may find normal eosinophil levels (Moore et al. 2010; Peters et al. 2010; Fitzpatrick and Moore 2017). An additional important observation from these clusters is that eosinophilic inflammation is evident also in non-allergic phenotypes. Late-onset asthma is mostly non-allergic and patients from this group may have high eosinophilic T2 inflammation, neutrophilic inflammation, or pauci-granulocytic inflammation (Opina and Moore 2017). In addition, obesity has a role in late-onset asthma with both eosinophilic and non-eosinophilic phenotypes (Kaur and Chupp 2019). Both the innate (natural killer cells and ILC2s) and adaptive (CD4+ T cells) immune systems can contribute to T2 and eosinophilic inflammation, with potentially variable contributions in each patient. The innate immune response is probably more dominant in the development of late-onset asthma symptoms, and this might explain why many eosinophilic patients are non-atopic. In summary, patients with SA may, as these studies suggest, belong to 3 clinically identifiable groups: (i) early-onset allergic disease (usually with high eosinophil counts), (ii) late-onset non-allergic with either eosinophilic predominant or (iii) neutrophilic (in sputum) inflammation (Moore et al. 2010; Opina and Moore 2017; Kaur and Chupp 2019). Severe T2 inflammation and eosinophilic asthma (both early and late-onset) have been associated with poor asthma control and more asthma exacerbations, and are therefore the center of various studies and encouraging new biological treatments (Tiotiu 2018; Kaur and Chupp 2019). Nevertheless, to date there are no specific biomarkers that can accurately predict the response to treatment in all patients. This opens a new research field of characterizing the sub-phenotype of the responders and the non-responders. The biology that underlies the non-T2 asthma phenotype is yet unclear, and we have very limited treatment options to suggest to this group of patients.
Pharmacological treatment for severe asthma
Steroids
ICS and LABA are the preferred controllers in all steps according to GINA guidelines (GINA 2019). While in some forms of asthma exacerbations a higher dose of ICS may be an effective treatment, SA patients usually need to add OCS. Furthermore, an estimated 24%–45% of patients with SA use systemic glucocorticoids to control the disease and prevent exacerbations (Schleich et al. 2014; Shaw et al. 2015). The need to control symptoms with a higher dose of steroids and the use of OCS in SA suggests that they are less sensitive to CS. The relative insensitivity in this group of patients might be a mechanism that contributes to asthma severity (Barnes and Adcock 2009). CS insensitivity has been associated with different comorbid conditions such as obesity, smoking, low vitamin D levels, and non-eosinophilic (low-TH2) inflammation (Barnes and Adcock 2009; Kaur and Chupp 2019). Oral glucocorticoid therapy has severe side effects and adversely affects health-related quality of life, therefore, there is a crucial need to look for effective alternative therapies. Few studies used immunosuppressive medications such as methotrexate, cyclosporine A, gold salts and IVIG as steroid sparing agents, and the results were uncertain while the adverse event profiles of some of these drugs are significant (Corrigan 2002).
Long acting muscarinic antagonist (LAMA)
LAMAs inhibit the muscarinic receptors of the bronchioles resulting in relaxation of the smooth muscle. Tiotropium bromide may also have other effects as it reduced airway inflammation and showed some negative effects on airway remodeling and hyper-responsiveness in a murine model of asthma (Ohta et al. 2010; Hamelmann 2018). LAMA showed a beneficial role in the treatment of patients with SA, and it is US Food and Drug Administration (FDA)-approved for the maintenance treatment of asthma in patients 6 years of age and older (FDA1 2004). Accordingly, the new GINA guidelines recommend using LAMA as an add-on therapy in step 4–5 patients (aged ≥6) that are not well controlled with ICS/LABA (GINA 2019). These current guidelines have based their recommendations on evidence from Phase III clinical studies investigating the use of tiotropium add-on therapy in SA. The PrimoTinA-asthma trial combined 2 replicate, randomized, controlled trials involving 912 patients with asthma that received either tiotropium (a total dose of 5 µg) or placebo, both delivered by a soft-mist inhaler once daily for 48 weeks (Kerstjens et al. 2012). All participants (18–75 years old) were symptomatic on inhaled glucocorticoids and LABAs, had a post-bronchodilator forced expiratory volume in 1 second (FEV1) of 80% or less of the predicted value, and had a history of at least 1 severe exacerbation in the previous year. The mean (±SE) change in both the pre-dose and peak FEV1 from baseline, at 24 weeks, was greater with tiotropium than with placebo in the 2 trials [88 ± 31 and 86 ± 34 mL in trial 1 (p = 0.01), 111 ± 30 and 154 ± 32 mL in trial 2 (p < 0.001)]. The addition of tiotropium increased the time to the first severe exacerbation (282 days vs. 226 days), with an overall reduction of 21% in the risk of a severe exacerbation (hazard ratio, 0.79; p = 0.03). The PrimoTinA-asthma trials provided some indication that tiotropium improves asthma symptom control, a secondary endpoint for the trials. The patients’ 7-question Asthma Control Questionnaire (ACQ-7) and the Asthma Quality of Life Questionnaire (AQLQ) scores in these trials did not achieve the minimal clinically important difference (a decrease in either score from baseline ≥0.5) (Kerstjens et al. 2012). However, in a post-hoc pooled analysis of both trials, ACQ-7 responder rate (the percent of patients achieving the minimal clinically important difference) was significantly higher at week 24 (OR 1.32, p = 0.04) and at week 48 (OR 1.68, p < 0.001) (Kerstjens et al. 2016). Importantly, these post-hoc subgroup analyses of PrimoTinA-asthma trials also demonstrated that add-on once-daily tiotropium 5 µg compared with placebo improved lung function, reduced the risk of asthma exacerbations and improved asthma symptom control, independent of a broad range of baseline characteristics (Kerstjens et al. 2016).
Phase III studies demonstrated the value of tiotropium add-on therapy also in the pediatric SA population. VivaTin A-asthma, a 12-week, double-blind, placebo-controlled trial assessed the efficacy and safety of once-daily tiotropium add-on therapy to high-dose ICS with 1 or more controller medications, or medium-dose ICS with 2 or more controller medications, in children with severe symptomatic asthma. The trial, involving 401 participants aged 6–11, demonstrated that add-on tiotropium 5 µg therapy significantly improved peak FEV1 (within 3 hours after dosing) and trough FEV1 compared with placebo [139 mL, (95% CI 75–203, p < 0.001), and 87mL (95% CI, 19–154; p = 0.01), respectively] (Szefler et al. 2017).
Four phase III trials, 2 in symptomatic moderate asthma (CanoTinA-asthma; RubaTinA-asthma) and 2 in symptomatic SA (VivaTinA-asthma; PensieTinA-asthma) demonstrated the efficacy and safety of tiotropium add-on therapy in 6–17-year-olds with symptomatic asthma (Hamelmann et al. 2016, 2017; Szefler et al. 2017, 2019). Most pediatric patients are allergic, raising the question of whether T2 inflammation influences the responsiveness to tiotropium add-on therapy. To address this question, Szefler and colleagues post-hoc analyzed the pooled data from these 4 randomized controlled trials (RCTs) to check whether there was a correlation between serum IgE levels and eosinophils counts, and the response to tiotropium. They found that the improvements in lung function, risk of exacerbations and improvement in ACQ responder rate were independent of T2 status of the patients (Szefler et al. 2019). Analyzing data from 4 adult phase III trials examining the same markers reached a similar result; tiotropium significantly reduced the risk of SA exacerbations and asthma worsening, regardless of T2 phenotype (Casale et al. 2018).
The results of all these studies in adults and pediatric patients demonstrate that tiotropium is effective across all asthma phenotypes. This suggests that tiotropium is a good add-on therapy option in patients with uncontrolled SA, irrespective of their subtype, before pursuing personalized biologic treatments (Hamelmann 2018).
Biologic treatment
Treatment targeting IgE
Omalizumab
Omalizumab was the first and only authorized biologic therapy for SA until 2015. The FDA approved it for use in moderate-to-severe allergic asthma in 2003 and the European Medicines Agency (EMA) in 2005. However, while very effective in moderate asthma, it is probably cost effective merely in SA, therefore, GINA guidelines recommend using it as add-on treatment for patients who are uncontrolled on step 4–5 (McQueen et al. 2018; GINA 2019). Patients with moderate asthma have other cost-effective add-on treatments like leukotriene antagonists or LAMA inhalers before the consideration of adding biologic treatments. For these reasons, in the following section, we will discuss the efficacy of omalizumab mainly in SA. Surprisingly, very few RCTs (5 out of 25, until 2014) studied the effects of omalizumab as an add-on treatment in patients above GINA step 4 (GINA step 5 or National Asthma Education and Prevention Program – Expert Panel Report 3 (NAEPP EPR-3) step 5 or 6) (National Heart, Lung, and Blood Institute 2007; Normansell et al. 2014). From these 5 studies, only 1 trial both investigated the clinical outcome and was published in a peer review journal. This study demonstrated that treating SAA patients with omalizumab for 48 weeks caused a 25% reduction in asthma exacerbations (PV 0.006) and improved asthma specific quality of life (Hanania et al. 2011). However, the study was not powered to detect the treatment effect of omalizumab in the OCS subgroup and could not show a steroid sparing effect.
Following the FDA approval of omalizumab, many “real-life” studies provided evidence of the effectiveness of omalizumab under conditions of greater heterogeneity and treatment patterns than the conditions in RCTs (Abraham et al. 2016; Tadrous et al. 2018). Nevertheless, it is very difficult to determine from these studies any conclusions about the efficacy of omalizumab treatment of SAA, since most of them were retrospective or observational studies, included patients with moderate asthma, and did not have a control group. For example, the 5-year EXCELS study, one of the biggest post marketing studies that included a control population, could not show any add-on benefit of omalizumab (Zazzali et al. 2015). This study summarized data on the quality of life and asthma control of moderate-to-severe persistent allergic asthma patients treated with omalizumab and those who did not receive omalizumab in a real-world setting. Patients who received omalizumab had virtually the same level of improvements in asthma control as were seen in those who did not receive the drug.
Most “real-life” retrospective studies that examined the improvement of SAA after starting omalizumab chose to include in the analysis only those patients who responded within 16 weeks to omalizumab. Usually, researchers compared asthma control between 2 periods, before omalizumab treatment and the period after treatment, without adding a control group. For instance, Mansur et al. collected data regarding the long-term efficacy and safety of omalizumab treatment from a severe asthma registry (Mansur et al. 2017). Out of all the patients in the registry, 169 met the criteria for SAA and 122 (72%) were on omalizumab therapy. While 100 patients (58%) were on long term omalizumab treatment, only 45 (26%) were included in the study. Importantly, there is no information on the outcome of the 42 (25%) patients who were not treated with omalizumab, the 5 patients who did not complete the 16 weeks at the time of the study, and on the 22 (13%) patients who discontinued omalizumab (Mansur et al. 2017). The data analysis of the 45 patients who were included showed a significant reduction in hospitalization, exacerbation, daily mean maintenance OCS dose (p < 0.0001), in addition to a clinically significant improvement in an asthma control questionnaire (ACQ). In summary, this study demonstrated that patients with SAA who initially responded sustained a good outcome with longer-term omalizumab therapy. However, in many “real life” studies, as in this study, the drop-out rate was relatively high compared to what was reported in RCTs and could reach up to 45.5%. In most post-marketing studies, lack of efficacy was responsible for treatment discontinuation while in RCTs it was usually the patients’ decision (Caminati et al. 2016). All these studies raise the following related and important questions: who responds to omalizumab, who does not, and why?
With the goal of approaching these questions, we collected from our Allergy and Immunology Clinic data on all patients who were on omalizumab treatment during 2006–2018. Therapy was started according to the Israel public drug program criteria for reimbursement of omalizumab for severe uncontrolled asthma. To be eligible a patient needed to fulfill all 4 criteria: (i) have uncontrolled GINA asthma step 4 in spite of maximal treatment (adherent to therapy with a proper technique), (ii) be a nonsmoker, with all other asthma-worsening conditions controlled, (iii) the request must be made by a specialist (respiratory or allergy and immunology) following a positive skin test reaction to a perennial aeroallergen, (iv) baseline IgE levels should be between 30–1500 IU/mL. In addition, the patient must have had at least 2 asthma exacerbations that required 2 courses of high-dose OCS in the preceding year unless there are contraindications for systemic steroid treatment (such as severe osteoporosis). We divided the patients into 2 groups: responders and non-responders. We defined a patient as a non-responder if he/she stopped omalizumab treatment at any time due to lack of efficacy. From 2006 through 2018, 48 patients started publicly funded omalizumab treatment in our clinic of whom 18 were responders, and 30 were non-responders (Table 1). As the results demonstrate, 63% (19 patients, 3 of them initially responded) of the non-responders were steroid dependent compared to only 5% (1 patient) in the responders group (p < 0.01). There was also a significant difference in the proportion with rhinitis between the 2 groups (94% in the responders compared to 30% in the non-responders, p < 0.05). When we collected our data, we in addition classified the patients as having either an allergic phenotype or a non-allergic phenotype (despite a positive skin test). The decision was made in agreement between 2 physicians. For example, a patient was considered allergic if he/she had early-onset asthma together with allergic type rhinitis (clear rhinorrhea with sneezing) and responded to exposure of a relevant perennial allergen. The results show very clearly that among the responders, there are significantly more patients with an allergic phenotype compared to the non-responders (89% vs. 26%, respectively, p < 0.01). In conclusion, this small survey suggests that omalizumab is most effective in a specific group of patients with uncontrolled severe truly allergic asthma and probably not steroid dependent. Our data were presented at the Israeli Association of Allergy and Clinical Immunology Annual Meeting in 2018 (p value was calculated using χ2 test).
Table 1:
Note: Data were significantly different for rhinitis (p < 0.05), allergy (p < 0.01), and steroid dependent state (<0.01). Our data were presented at the Israeli Association of Allergy and Clinical Immunology Annual Meeting in 2018. p value was calculated using χ2 test.
a
3 steroid dependent patients initially responded.
Treatment targeting IL-5
Mepolizumab, Reslizumab, and Benralizumab
The FDA approved 3 anti-IL-5 biologic treatments for severe eosinophilic asthma (SEA) (See Table 2). Mepolizumab and reslizumab were approved as add-on therapies in 2015 and 2016, respectively. Both are monoclonal antibodies that bind directly to IL-5, thus preventing the association between IL-5 and the alpha chain of the IL-5 receptor on eosinophils and basophils. Benralizumab is the most recently FDA-approved anti-IL-5 (2017) drug. Benralizumab differs from the other anti-IL-5 drugs in that it directly binds the IL-5-alpha receptor expressed on the surface of eosinophils and basophils, thus preventing IL-5 from binding to the alpha-receptor. Benralizumab binding also results in death of eosinophils and basophils via antibody-dependent cell-mediated cytotoxicity (Krings et al. 2019). Overall, there is very good data evidence that supports the use of all anti-IL-5 treatments as an adjunct to standard of care in people with SEA that is poorly controlled. A recent Cochrane (2017) review found that anti-IL-5 treatment approximately halves the rate of asthma exacerbations in this population (Farne et al. 2017). All anti-IL-5 treatments produced a small but statistically significant improvement in mean pre-bronchodilator FEV1 of between 0.08 L and 0.11 L.
Table 2:
The FDA did not set a specific blood eosinophil threshold required for usage of any of the different anti-IL-5 drugs. Nevertheless, reslizumab studies included patients with an induced sputum eosinophil count of ≥3% or blood eosinophil count of ≥400 cells/µL, therefore, blood eosinophil cut off of ≥400 cells/µL is usually used clinically (Maselli et al. 2016). For both mepolizumab and benralizumab, the primary end point was based on patients with an absolute eosinophil count of greater than or equal to 300 cells/µL. In both biologics, improvements in exacerbation frequency did occur in patients with SA with a blood eosinophil count of 150–300 cells/µL (Bleecker et al. 2016; FitzGerald et al. 2016; Ortega et al. 2016). If a patient is on chronic OCS, the steroids may reduce blood eosinophil levels; consequently, the recommended eosinophil threshold in this subpopulation is ≥150 cells/µL (FitzGerald et al. 2018; Krings et al. 2019).
Aside from blood eosinophil counts, what can also predict a positive response to anti-IL-5? Analysis of the 2 randomized, double-blind, placebo-controlled SIROCCO and CALIMA phase III studies showed that the predictors of response to benralizumab include OCS use, history of nasal polyposis, reduced lung function (forced vital capacity <65% predicted), 3 or more exacerbations in the previous year, age 18 years or more, and a high basal eosinophil count (Bleecker et al. 2018). More studies are needed to determine these predictors for the other anti-IL-5 drugs.
Few studies showed the efficacy of anti-IL-5 as steroid sparing in SEA patients requiring chronic OCS. The SIRIUS (Steroid Reduction with Mepolizimab Study) trial evaluated the effect of mepolizumab treatment in patients with chronic blood eosinophilia despite the daily use of systemic CS. This study showed that patients who received the drug were able to reduce their OCS dosage by 50%, and 14% could completely discontinue their OCS (Bel et al. 2014). The ZONDA trial tested the efficacy of benralizumab to reduce OCS use in patients with uncontrolled asthma and chronic OCS. This study clearly demonstrated a steroid sparing effect of benralizumab. Patients receiving the drug were able to reduce their OCS dose by 75%, and 52% were able to discontinue OCS (Nair et al. 2017). Adults were eligible to participate in the ZONDA study if they had a blood eosinophil count of at least 150 cells/mm3. Interestingly, the baseline eosinophil counts in patients who did not show a response to benralizumab were similar to those in patients who showed the greatest reductions in their final OCS doses (Nair et al. 2017). This suggests that in patients on OCS, the levels of blood eosinophils may not predict the response to benralizumab.
Dupilumab
Dupilumab is a fully human monoclonal antibody to the IL-4 receptor alpha subunit that inhibits both IL-4 and IL-13 signaling and hence T2 inflammation (Wenzel et al. 2013). The FDA approved it for use in patients aged 12 years and older with an eosinophilic phenotype or with OCS dependent asthma (Table 2).
Two recent phase III double blind RCTs have shown the efficacy of dupilumab for the treatment of moderate to severe asthma inadequately controlled with ICS and LABA (Castro et al. 2018; Rabe et al. 2018). Both studies recruited patients with no minimum requirement regarding baseline blood or sputum eosinophil counts or any other T2 biomarkers (i.e., FeNO or IgE). In the QUEST (Evaluation of Dupilumab in Patients with Persistent Asthma Study) trial, patients receiving dupilumab subcutaneously (200 or 300 mg every 2 weeks) had about 50% less severe asthma exacerbation during the 52 trial weeks compared to their matched placebo. Pre-specified subgroup analyses according to blood eosinophil count showed significant differences between the dupilumab and placebo groups in exacerbation rates in patients with ≥150 eosinophils at baseline, but not with eosinophil counts of <150 cells/µL (Castro et al. 2018). Interestingly, patients with an elevated FeNO level of 25 ppb or greater irrespective of their blood eosinophil levels had 61%–65% reduction in asthma exacerbations (Castro et al. 2018). This finding suggests that dupilumab may be effective in severe asthmatic patients with high FeNO levels and normal blood eosinophils.
The VENTURE (Evaluation of Dupilumab in Patients with Severe Steroid Dependent Asthma Study) trial specifically examined the effect of dupilumab in OCS dependent asthmatic patients (Rabe et al. 2018). The net percentage reduction in the glucocorticoid dose was 30% more in the dupilumab group, as compared to the placebo group and 23% more patients within the treatment group completely discontinued OCS use. Importantly, despite the lower steroid dose dupilumab treatment resulted in a 59% reduction in severe exacerbation rate compared to that in the placebo group and an FEV1 that was 0.22 L higher (Rabe et al. 2018). Unlike with anti-IL-5 therapies, the effect of dupilumab in patients with steroid dependent asthma was unrelated to the baseline blood eosinophil levels, and resulted in reduced FeNO levels, suggesting that dupilumab inhibits T2 inflammation more broadly than targeting eosinophils alone. Importantly, the FDA also approved dupilumab as add-on maintenance treatment in adult patients with chronic rhinosinusitis with nasal polyposis (CRSwNP) making it an attractive treatment for patients who suffer from both SA and CRSwNP (FDA6 2017).
Treatment to be considered in non-T2 inflammation SA
Bronchial thermoplasty
Bronchial thermoplasty (BT) is an invasive procedure that delivers radiofrequency thermal energy to the airway wall. It is usually performed in 3 bronchoscopy sessions 2–3 weeks apart (Tan et al. 2019). The FDA first approved BT in 2010 following the Asthma Intervention Research 2 (AIR2) study, a multicenter, double blind, randomized, sham bronchoscopy controlled trial (FDA7 2010). It was approved for the treatment of persistent SA in patients 18 years and older whose asthma is not well controlled with ICS and LABA (Castro et al. 2010). The AIR2 study showed a modest improvement in Asthma Quality of Life Questionnaire (AQLQ). While there were more adverse events in the BT groups during the 6 week treatment period (including more hospitalizations), in the post treatment period (6–52 weeks following treatment) the BT group experienced fewer severe exacerbations, emergency department (ED) visits, and days missed from work/school compared with the placebo group (Castro et al. 2010). A continuation study, following the same subjects for up to 5 years after treatment, showed that severe exacerbation rates and ER visit rates remained similar in years 2–5 as compared to year 1 after BT and were lower than the year before BT (Wechsler et al. 2013).
The ERS/ATS guidelines from 2014 recommend that BT be performed in adults with SA only in the context of an Institutional Review Board (IRB)-approved independent systematic registry or a clinical study because of potential adverse events and lack of understanding of the phenotype of patients that may benefit from this procedure. Specifically, the ERS/ATS called for additional studies with different primary outcomes, such as exacerbation rates. In addition, they expressed the need to better describe the phenotypes of the responding patients, the effects in patients with severe obstructive asthma (FEV1 <60% of predicted value) and in patients using systemic CS, together with long-term benefits and safety (Chung et al. 2014). The more recent SA guidelines from GINA 2019 recommend considering BT with registry enrollment in SA patients who have no evidence of T2 inflammation, or if a patient has not responded to T2 targeted therapy (GINA 2019).
Macrolides
Macrolide antibiotic therapy at low doses is a non-specific treatment that is used in several respiratory conditions, even without an infection. Macrolides have been shown to have additional non-antibiotic properties, such as anti-inflammatory, immunomodulatory, reduction in mucus production, and anti-viral activities (Ribeiro et al. 2009; Zimmermann et al. 2009; Gielen et al. 2010; Spagnolo et al. 2013). Administration of macrolides in SA has not been shown to provide a consistent benefit. In a Cochrane database systematic review, conducted in 2015, Kew et al. examined 23 RCTs that treated chronic asthma (adults and children) with at least 4 weeks of macrolides. They described the quality of evidence as being generally very low. Most of the studies included SA patients, although inclusion criteria varied between the studies. Macrolides were not shown to be better than placebo for most of the clinical outcomes, including exacerbations requiring hospitalization or OCS, symptom scales, asthma control, quality of life and rescue medication use. The review notes 2 within-study subgroup analyses that indicate there may be a beneficial effect in non-eosinophilic asthma (Kew et al. 2015). In an individual participant data meta-analysis from 2019, Hiles et al. examined RCTs that compared at least 8 weeks of azithromycin with placebo in the adult population. The number of exacerbations was assessed for at least 6 months. The goal of the study was to test the efficacy of azithromycin in reducing exacerbations in asthma, and examining the sub-phenotypes of non-eosinophilic asthma, eosinophilic asthma and SA. Three studies met the inclusion criteria and indicated that azithromycin was associated with a lower exacerbation rate for all patients and for the sub-phenotypes. Specifically, patients with eosinophilic asthma exhibited less OCS use, and patients with non-eosinophilic asthma exhibited less antibiotic use (Hiles et al. 2019).
One of the main concerns about macrolide use is the development of resistant microorganisms. The AZISAST study, which examined patients with SA treated for 6 months with either azithromycin or placebo, showed that azithromycin was well tolerated but associated with increased oropharyngeal carriage of macrolide-resistant Streptococci. During the 4-week washout period, the percentage of macrolide-resistant Streptococci decreased (Brusselle et al. 2013). A sub-study of the AZISAST study examined the oropharyngeal microbiome by using a cultivation-independent method using next-generation sequencing of amplified 16S rRNA genes. This sub-study showed that the microbiome of severe asthmatics is similar to healthy individuals, and the 6 months of azithromycin administration increased Streptococcus salivarius approximately 5-fold and decreased Leptotrichia wadei approximately 5-fold. In this study, 4 of the 8 patients regained their initial bacterial composition within 1 month after cessation of the treatment (Lopes Dos Santos Santiago et al. 2017). An additional study from 2019 examined the 16S rRNA sequencing and quantitative PCR in the sputum of patients treated with either azithromycin or placebo for 48 weeks. This study also showed an increase in macrolide resistance in addition to reduced airway Haemophilus influenzae load (Taylor et al. 2019). These studies showing increased resistance in patients chronically treated with macrolides question the long-term safety of this class of drugs as a treatment option for SA patients.
Due to the low level of evidence and the potential of creating resistant bacteria, the ERS/ATS guidelines do not recommend the use of macrolides in SA. The most current GINA recommendations mention macrolides as an off-label treatment option for patients with no T2 inflammation evidence, or patients who did not respond to any T2 targeted therapy (GINA 2019).
Summary and conclusions
Management of uncontrolled SA is becoming more challenging. On the one hand, new biologic treatments are available; on the other hand, the expense is growing significantly. The ideal aim of efficient precision medicine is to define for each medication the patient population that is most likely to respond, and to reduce the chance of therapy failure. In our clinic, we found that patients who responded to omalizumab showed a truly allergic phenotype, and were less likely to be steroid dependent. Based on these findings and the current knowledge, we have attempted to create a suggested algorithm to aid in the selection of treatments for uncontrolled SA patients (Figure 1).
Figure 1:
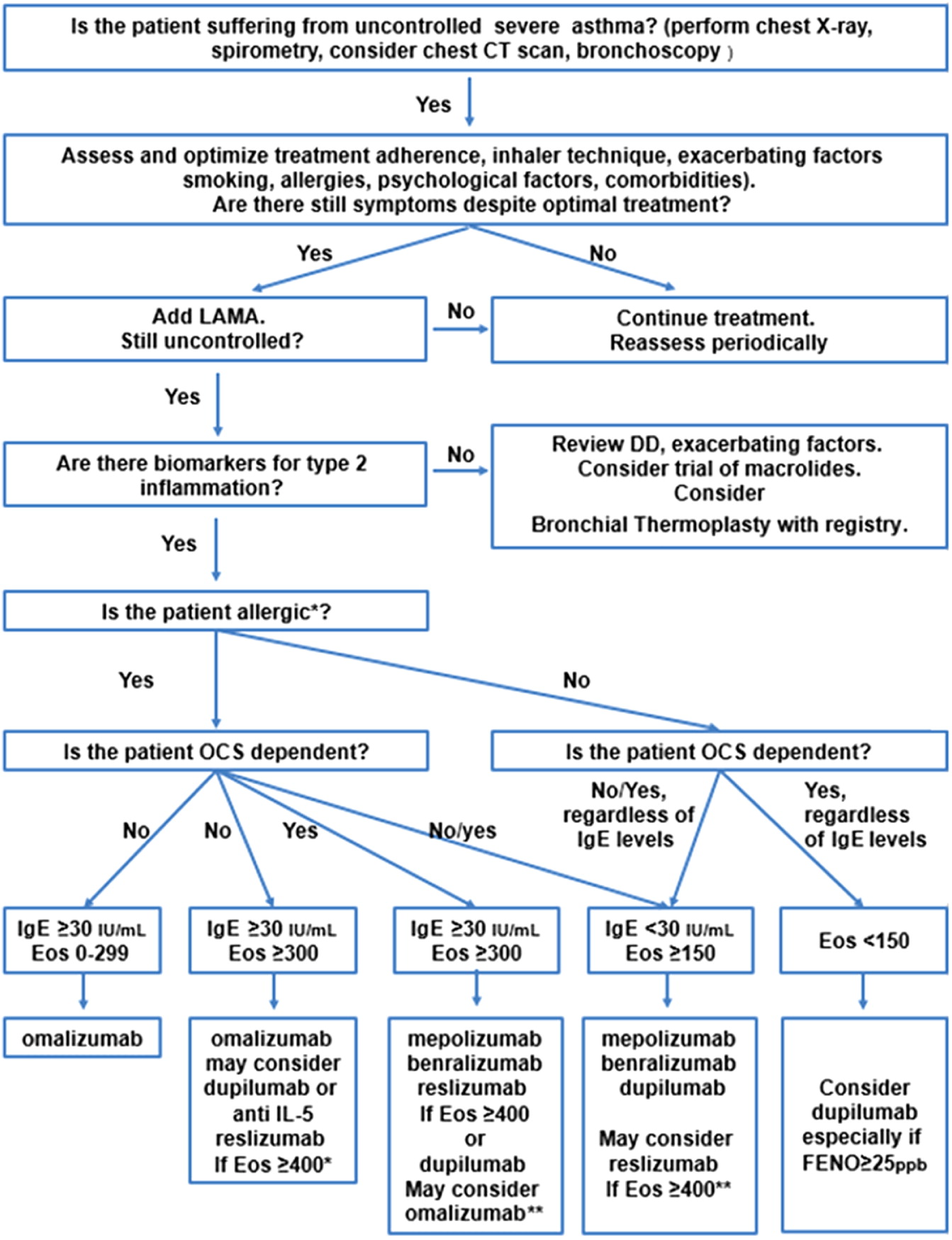
However, more research is necessary in order to provide accurate guidance regarding the selection of specific biologics. Several questions are yet unanswered, for example, what is the best biologic treatment for a truly allergic SA patient who is steroid dependent despite LAMA add-on therapy and has an elevated eosinophil count? In addition, out of all the available biological therapeutics, which one is the best for eosinophilic SA patients?
These questions can be addressed by head-to-head RCTs comparing the different biologics in the specific patient groups. Meanwhile, since such studies are not yet underway, we have to invest in the characterization of the responders without omitting those who do not respond, despite meeting the criteria to be eligible for the specific treatment. Learning the characteristics of these populations may help us develop the clinical tools and markers for more efficient precision medicine for uncontrolled SA in the future.
Acknowledgement
We would like to thank our colleagues Dr Nusam David, Dr Panasoff Josef, and Nizar Abu Hilo for their contribution to our clinic’s retrospective study.
REFERENCES
Abraham I., Alhossan A., Lee C.S., Kutbi H., and MacDonald K. 2016. ‘Real-life’ effectiveness studies of omalizumab in adult patients with severe allergic asthma: Systematic review. Allergy. 71:593–610.
Aron J.L. and Akbari O. 2017. Regulatory T cells and type 2 innate lymphoid cell-dependent asthma. Allergy. 72:1148–1155.
Barnes P.J. and Adcock I.M. 2009. Glucocorticoid resistance in infl ammatory disease. Lancet. 373:1905–1917.
Bel E.H., Wenzel S.E., Thompson P.J., Prazma C.M., Keene O.N., Yancey S.W., Ortega H.G., and Pavord I.D. 2014. Oral glucocorticoid-sparing effect of mepolizumab in eosinophilic asthma. N. Engl. J. Med. 371:1189–1197.
Berkman N., Avital A., Breuer R., Bardach E., Springer C., and Godfrey S. 2005. Exhaled nitric oxide in the diagnosis of asthma: Comparison with bronchial provocation tests. Thorax. 60:383–388.
Bleecker E.R., FitzGerald J.M., Chanez P., Papi A., Weinstein S.F., Barker P., Sproule S., Gilmartin G., Aurivillius M., Werkström V., and Goldman M. 2016. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β2-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 388:2115–2127.
Bleecker E.R., Wechsler M.E., Mark FitzGerald J., Menzies-Gow A., Wu Y., Hirsch I., Goldman M., Newbold P., and Zangrilli J.G. 2018. Baseline patient factors impact on the clinical efficacy of benralizumab for severe asthma. Eur. Respir. J. 52:1800936.
Bousquet J., Mantzouranis E., Cruz A.A., Aït-Khaled N., Baena-Cagnani C.E., Bleecker E.R., Brightling C.E., Burney P., Bush A., Busse W.W., Casale T.B., Chan-Yeung M., Chen R., Chowdhury B., Chung K.F., Dahl R., Drazen J.M., Fabbri L.M., Holgate S.T., Kauffmann F., Haahtela T., Khaltaev N., Kiley J.P., Masjedi M.R., Mohammad Y., O’Byrne P., Partridge M.R., Rabe K.F., Togias A., Van Weel C., Wenzel S., Zhong N., and Zuberbier T. 2010. Uniform definition of asthma severity, control, and exacerbations: Document presented for the World Health Organization Consultation on Severe Asthma. J. Allergy Clin. Immunol. 126:926–938.
Brusselle G.G., VanderStichele C., Jordens P., Deman R., Slabbynck H., Ringoet V., Verleden G., Demedts I.K., Verhamme K., Delporte A., Demeyere B., Claeys G., Boelens J., Padalko E., Verschakelen J., Van Maele G., Deschepper E., and Joos G.F.P. 2013. Azithromycin for prevention of exacerbations in severe asthma (AZISAST): A multicentre randomised double-blind placebo-controlled trial. Thorax. 68:322–329.
Busse W.W. 2019. Biological treatments for severe asthma: A major advance in asthma care. Allergol. Int. 68:158–166.
Caminati M., Senna G., Stefanizzi G., Bellamoli R., Longhi S., Chieco-Bianchi F., Guarnieri G., Tognella S., Olivieri M., Micheletto C., Festi G., Bertocco E., Mazza M., Rossi A., and Vianello A. 2016. Drop-out rate among patients treated with omalizumab for severe asthma: Literature review and real-life experience. BMC Pulm. Med. 16:1–9.
Carr T.F. and Kraft M. 2017. Management of severe asthma before referral to the severe asthma specialist. J. Allergy Clin. Immunol. Pract. 5:877–886.
Casale T.B., Bateman E.D., Vandewalker M., Virchow J.C., Schmidt H., Engel M., Moroni-Zentgraf P., and Kerstjens H.A.M. 2018. Tiotropium respimat add-on is efficacious in symptomatic asthma, independent of T2 Phenotype. J. Allergy Clin. Immunol. Pract. 6:923–935.
Castro M., Rubin A., Laviolette M., Fiterman J., de Andrade Lima M., and Shah P. 2010. Asthma intervention research 2 (AIR2) trial. Am. J. Respir. Crit. Care Med. 181:116–124.
Castro M., Corren J., Pavord I.D., Maspero J., Wenzel S., Rabe K.F., Busse W.W., Ford L., Sher L., FitzGerald J.M., Katelaris C., Tohda Y., Zhang B., Staudinger H., Pirozzi G., Amin N., Ruddy M., Akinlade B., Khan A., Chao J., Martincova R., Graham N.M.H., Hamilton J.D., Swanson B.N., Stahl N., Yancopoulos G.D., and Teper A. 2018. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N. Engl. J. Med. 378:2486–2496.
Chen R., Smith S.G., Salter B., El-Gammal A., Oliveria J.P., Obminski C., Watson R., O’Byrne P.M., Gauvreau G.M., and Sehmi R. 2017. Allergen-induced increases in sputum levels of group 2 innate lymphoid cells in subjects with asthma. Am. J. Respir. Crit. Care Med. 196:700–712.
Chung K.F., Wenzel S.E., Brozek J.L., Bush A., Castro M., Sterk P.J., Adcock I.M., Bateman E.D., Bel E.H., Bleecker E.R., Boulet L.P., Brightling C., Chanez P., Dahlen S.E., Djukanovic R., Frey U., Gaga M., Gibson P., Hamid Q., Jajour N.N., Mauad T., Sorkness R.L., and Teague W.G. 2014. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 43:343–373.
Corrigan C.J. 2002. Asthma refractory to glucocorticoids: The role of newer immunosuppressants. Am. J. Respir. Med. 1:47–54.
De Groot J.C., Brinke A., Ten, and Bel E.H.D. 2015. Management of the patient with eosinophilic asthma: A new era begins. ERJ Open Res. 1:00024-2015.
Dweik R.A., Boggs P.B., Erzurum S.C., Irvin C.G., Leigh M.W., Lundberg J.O., Olin A.C., Plummer A.L., and Taylor D.R. 2011. An official ATS clinical practice guideline: Interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am. J. Respir. Crit. Care Med. 184:602–615.
Fahy J. V. 2015. Type 2 inflammation in asthma-present in most, absent in many. Nat. Rev. Immunol. 15:57–65.
Farne H.A., Wilson A., Powell C., Bax L., and Milan S.J. 2017. Anti-IL5 therapies for asthma. Cochrane Database Syst. Rev. 9:CD010834.
FDA1. 2004, revised February 2019. Highlights of prescribing information for SPIRIVA RESPIMAT. [Online]. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021936s012lbl.pdf [accessed October 2019].
FDA2. 2003, revised May 2019. Highlights of prescribing information for XOLAIR. [Online]. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/103976s5234lbl.pdf [accessed October 2019].
FDA3. 2015, revised September 2019. Highlights of prescribing information for NUCALA. [Online]. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/125526s012,761122s002s003lbl.pdf [accessed October 2019].
FDA4. 2016, revised January 2019. Highlights of prescribing information for CINQAIR. [Online]. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/0761033s010lbl.pdf [accessed October 2019].
FDA5. 2017, revised October 2019. Highlights of prescribing information for FASENRA. [Online]. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761070s005lbl.pdf [accessed October 2019].
FDA6. 2017, revised June 2019. Highlights of prescribing information for DUPIXENT. [Online]. Available from https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761055s014lbl.pdf [accessed October 2019].
FDA7. 27 April 2010. Premarket approval (PMA) of Alair bronchial thermoplasty system. [Online]. Available from https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P080032 [accessed October 2019].
FitzGerald J.M., Bleecker E.R., Nair P., Korn S., Ohta K., Lommatzsch M., Ferguson G.T., Busse W.W., Barker P., Sproule S., Gilmartin G., Werkström V., Aurivillius M., and Goldman M. 2016. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 388:2128–2141.
FitzGerald J.M., Bleecker E.R., Menzies-Gow A., Zangrilli J.G., Hirsch I., Metcalfe P., Newbold P., and Goldman M. 2018. Predictors of enhanced response with benralizumab for patients with severe asthma: pooled analysis of the SIROCCO and CALIMA studies. Lancet Respir. Med. 6:51–64.
Fitzpatrick A.M. and Moore W.C. 2017. Severe asthma phenotypes — How should they guide evaluation and treatment? J. Allergy Clin. Immunol. Pract. 5:901–908.
Gielen V., Johnston S.L., and Edwards M.R. 2010. Azithromycin induces anti-viral responses in bronchial epithelial cells. Eur. Respir. J. 36:646–654.
GINA. 2019. Global strategy for asthma management and prevention (2019 update). [Online]. Available from https://ginasthma.org/wp-content/uploads/2019/06/GINA-2019-main-report-June-2019-wms.pdf [accessed October 2019].
Good J.T., Kolakowski C.A., Groshong S.D., Murphy J.R., and Martin R.J. 2012. Refractory asthma: Importance of bronchoscopy to identify phenotypes and direct therapy. Chest. 141:599–606.
Haldar, P., Pavord, I.D., Shaw, D.E., Berry, M.A., Thomas, M., Brightling, C.E., Wardlaw, A.J., and Green, R.H. 2008. Cluster analysis and clinical asthma phenotypes. Am. J. Respir. Crit. Care Med.
Hamelmann E. 2018. Managing severe asthma: A role for the long-acting Muscarinic Antagonist Tiotropium. Biomed Res. Int. 2018:1–9.
Hamelmann E., Bateman E.D., Vogelberg C., Szefler S.J., Vandewalker M., Moroni-Zentgraf P., Avis M., Unseld A., Engel M., and Boner A.L. 2016. Tiotropium add-on therapy in adolescents with moderate asthma: A 1-year randomized controlled trial. J. Allergy Clin. Immunol. 138:441–450.
Hamelmann E., Bernstein J.A., Vandewalker M., Moroni-Zentgraf P., Verri D., Unseld A., Engel M., and Boner A.L. 2017. A randomised controlled trial of tiotropium in adolescents with severe symptomatic asthma. Eur. Respir. J. 49:1601100.
Hanania N.A., Alpan O., Hamilos D.L., Condemi J.J., Reyes-Rivera I., Zhu J., Rosen K.E., Eisner M.D., Wong D.A., and Busse W. 2011. Omalizumab in severe allergic asthma inadequately controlled with standard therapy: A randomized trial. Ann. Intern. Med. 154:573–582.
Hanania N.A., Korenblat P., Chapman K.R., Bateman E.D., Kopecky P., Paggiaro P., Yokoyama A., Olsson J., Gray S., Holweg C.T.J., Eisner M., Asare C., Fischer S.K., Peng K., Putnam W.S., and Matthews J.G. 2016. Efficacy and safety of lebrikizumab in patients with uncontrolled asthma (LAVOLTA I and LAVOLTA II): Replicate, phase 3, randomised, double-blind, placebo-controlled trials. Lancet Respir. Med. 4:781–796.
Hazenberg M.D. and Spits H. 2014. Human innate lymphoid cells. Blood. 124:700–709.
Hiles, S.A., McDonald, V.M., Guilhermino, M., Brusselle, G.G., and Gibson, P.G. 2019. Does maintenance azithromycin reduce asthma exacerbations? An individual participant data meta-analysis. Eur. Respir. J.
Hirose K., Iwata A., Tamachi T., and Nakajima H. 2017. Allergic airway inflammation: Key players beyond the Th2 cell pathway. Immunol. Rev. 278:145–161.
Hoyte F.C.L., Gross L.M., and Katial R.K. 2018. Exhaled nitric oxide: An update. Immunol. Allergy Clin. North Am. 38:573–585.
Inoue Y., Izuhara K., Ohta S., Ono J., and Shimojo N. 2015. No increase in the serum periostin level is detected in elementary school-age children with allergic diseases. Allergol. Int. 64:289–290.
Izuhara K., Conway S.J., Moore B.B., Matsumoto H., Holweg C.T.J., Matthews J.G., and Arron J.R. 2016. Roles of periostin in respiratory disorders. Am. J. Respir. Crit. Care Med. 193:949–956.
Jatakanon A., Lim S., and Barnes P.J. 2000. Changes in sputum eosinophils predict loss of asthma control. Am. J. Respir. Crit. Care Med. 161:64–72.
Kaur R. and Chupp G. 2019. Phenotypes and endotypes of adult asthma: Moving toward precision medicine. J. Allergy Clin. Immunol. 144:1–12.
Kerstjens H.A.M., Engel M., Dahl R., Paggiaro P., Beck E., Vandewalker M., Sigmund R., Seibold W., Moroni-Zentgraf P., and Bateman E.D. 2012. Tiotropium in asthma poorly controlled with standard combination therapy. N. Engl. J. Med. 367:1198–1207.
Kerstjens H.A.M., Moroni-Zentgraf P., Tashkin D.P., Dahl R., Paggiaro P., Vandewalker M., Schmidt H., Engel M., and Bateman E.D. 2016. Tiotropium improves lung function, exacerbation rate, and asthma control, independent of baseline characteristics including age, degree of airway obstruction, and allergic status. Respir. Med. 117:198–206.
Kew K.M., Undela K., Kotortsi I., and Ferrara G. 2015. Macrolides for chronic asthma. Cochrane Database Syst Rev. 15: CD002997.
Kharitonov S.A., Yates D., Robbins R.A., Barnes P.J., Logan-Sinclair R., and Shinebourne E.A. 1994. Increased nitric oxide in exhaled air of asthmatic patients. Lancet. 343:133–135.
Krings J.G., McGregor M.C., Bacharier L.B., and Castro M. 2019. Biologics for severe asthma: Treatment-specific effects are important in choosing a specific agent. J. Allergy Clin. Immunol. Pract. 7:1379–1392.
Lang D.M. 2015. Severe asthma: Epidemiology, burden of illness, and heterogeneity. Allergy Asthma Proc. 36:418–424.
Lefaudeux D., De Meulder B., Loza M.J., Peffer N., Rowe A., Baribaud F., Bansal A.T., Lutter R., Sousa A.R., Corfield J., Pandis I., Bakke P.S., Caruso M., Chanez P., Dahlén S.E., Fleming L.J., Fowler S.J., Horvath I., Krug N., Montuschi P., Sanak M., Sandstrom T., Shaw D.E., Singer F., Sterk P.J., Roberts G., Adcock I.M., Djukanovic R., Auffray C., Chung K.F., Adriaens N., Ahmed H., Aliprantis A., Alving K., Badorek P., Balgoma D., Barber C., Bautmans A., Behndig A.F., Bel E., Beleta J., Berglind A., Berton A., Bigler J., Bisgaard H., Bochenek G., Boedigheimer M.J., Bøonnelykke K., Brandsma J., Braun A., Brinkman P., Burg D., Campagna D., Carayannopoulos L., Carvalho da Purfição Rocha J.P., Chaiboonchoe A., Chaleckis R., Coleman C., Compton C., D’Amico A., Dahlén B., De Alba J., de Boer P., De Lepeleire I., Dekker T., Delin I., Dennison P., Dijkhuis A., Draper A., Edwards J., Emma R., Ericsson M., Erpenbeck V., Erzen D., Faulenbach C., Fichtner K., Fitch N., Flood B., Frey U., Gahlemann M., Galffy G., Gallart H., Garret T., Geiser T., Gent J., Gerhardsson de Verdier M., Gibeon D., Gomez C., Gove K., Gozzard N., Guo Y.K., Hashimoto S., Haughney J., Hedlin G., Hekking P.P., Henriksson E., Hewitt L., Higgenbottam T., Hoda U., Hohlfeld J., Holweg C., Howarth P., Hu R., Hu S., Hu X., Hudson V., James A.J., Kamphuis J., Kennington E.J., Kerry D., Klüglich M., Knobel H., Knowles R., Knox A., Kolmert J., Konradsen J., Kots M., Krueger L., Kuo S., Kupczyk M., Lambrecht B., Lantz A.S., Larsson L., Lazarinis N., Lone-Satif S., Marouzet L., Martin J., Masefield S., Mathon C., Matthews J.G., Mazein A., Meah S., Maiser A., Menzies-Gow A., Metcalf L., Middelveld R., Mikus M., Miralpeix M., Monk P., Mores N., Murray C.S., Musial J., Myles D., Naz S., Nething K., Nicholas B., Nihlen U., Nilsson P., Nordlund B., Östling J., Pacino A., Pahus L., Palkonnen S., Pavlidis S., Pennazza G., Petrén A., Pink S., Postle A., Powel P., Rahman-Amin M., Rao N., Ravanetti L., Ray E., Reinke S., Reynolds L., Riemann K., Riley J., Robberechts M., Roberts A., Rossios C., Russell K., Rutgers M., Santini G., Sentoninco M., Schoelch C., Schofield J.P.R., Seibold W., Sigmund R., Sjödin M., Skipp P.J., Smids B., Smith C., Smith J., Smith K.M., Söderman P., Sogbesan A., Staykova D., Strandberg K., Sun K., Supple D., Szentkereszty M., Tamasi L., Tariq K., Thörngren J.O., Thornton B., Thorsen J., Valente S., van Aalderenm W., van de Pol M., van Drunen K., van Geest M., Versnel J., Vestbo J., Vink A., Vissing N., von Garnier C., Wagerner A., Wagers S., Wald F., Walker S., Ward J., Weiszhart Z., Wetzel K., Wheelock C.E., Wiegman C., Williams S., Wilson S.J., Woosdcock A., Yang X., Yeyashingham E., Yu W., Zetterquist W., and Zwinderman K. 2017. U-BIOPRED clinical adult asthma clusters linked to a subset of sputum omics. J. Allergy Clin. Immunol. 139:1797–1807.
Leuppi J.D., Salome C.M., Jenkins C.R., Anderson S.D., Xuan W., Marks G.B., Koskela H., Brannan J.D., Freed R., Andersson M., Chan H.K., and Woolcock A.J. 2001. Predictive markers of asthma exacerbation during stepwise dose reduction of inhaled corticosteroids. Am. J. Respir. Crit. Care Med. 163:406–412.
Li N., Qiu R., Yang Z., Li J., Chung K.F., Zhong N., and Zhang Q. 2017. Sputum microbiota in severe asthma patients: Relationship to eosinophilic inflammation. Respir. Med. 131:192–198.
Lopes Dos Santos Santiago G., Brusselle G., Dauwe K., Deschaght P., Verhofstede C., Vaneechoutte D., Deschepper E., Jordens P., Joos G., and Vaneechoutte M. 2017. Influence of chronic azithromycin treatment on the composition of the oropharyngeal microbial community in patients with severe asthma. BMC Microbiol. 17:1–12.
Mansur A.H., Srivastava S., Mitchell V., Sullivan J., and Kasujee I. 2017. Longterm clinical outcomes of omalizumab therapy in severe allergic asthma: Study of efficacy and safety. Respir. Med. 124:36–43.
Maselli D.J., Velez M.I., and Rogers L. 2016. Reslizumab in the management of poorly controlled asthma: The data so far. J. Asthma Allergy 9:155–162.
McBrien C.N. and Menzies-Gow A. 2017. The biology of eosinophils and their role in asthma. Front. Med. 4:93.
McQueen R.B., Sheehan D.N., Whittington M.D., van Boven J.F.M., and Campbell J.D. 2018. Cost-effectiveness of biological asthma treatments: A systematic review and recommendations for future economic evaluations. Pharmacoeconomics. 36:957–971.
Medrek S.K., Parulekar A.D., and Hanania N.A. 2017. Predictive biomarkers for asthma therapy. Curr. Allergy Asthma Rep. 17:69.
Mitchell P.D. and O’Byrne P.M. 2017. Epithelial-derived cytokines in asthma. Chest. 151:1338–1344.
Moore W.C., Meyers D.A., Wenzel S.E., Teague W.G., Li H., Li X., D’Agostino R., Castro M., Curran-Everett D., Fitzpatrick A.M., Gaston B., Jarjour N.N., Sorkness R., Calhoun W.J., Chung K.F., Comhair S.A.A., Dweik R.A., Israel E., Peters S.P., Busse W.W., Erzurum S.C., and Bleecker E.R. 2010. Identification of asthma phenotypes using cluster analysis in the severe asthma research program. Am. J. Respir. Crit. Care Med. 181:315–323.
Moore W.C., Evans M.D., Bleecker E.R., Busse W.W., Calhoun W.J., Castro M., Chung K.F., Erzurum S.C., Curran-Everett D., Dweik R.A., Gaston B., Hew M., Israel E., Mayse M.L., Pascual R.M., Peters S.P., Silveira L., Wenzel S.E., and Jarjour N.N. 2011. Safety of investigative bronchoscopy in the Severe Asthma Research Program. J. Allergy Clin. Immunol. 128:328–336.e3.
Nair P., Wenzel S., Rabe K.F., Bourdin A., Lugogo N.L., Kuna P., Barker P., Sproule S., Ponnarambil S., and Goldman M. 2017. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N. Engl. J. Med. 376:2448–2458.
National Heart, Lung, and Blood Institute. 2007. National asthma education and prevention program: Expert panel report III: Guidelines for the diagnosis and management of asthma. J Allergy Clin Immunol. 120:S94–S138.
Normansell R., Walker S., Milan S.J., Walters E.H., and Nair P. 2014. Omalizumab for asthma in adults and children. Cochrane Database Syst. Rev. 13: CD003559.
Ohta S., Oda N., Yokoe T., Tanaka A., Yamamoto Y., Watanabe Y., Minoguchi K., Ohnishi T., Hirose T., Nagase H., Ohta K., and Adachi M. 2010. Effect of tiotropium bromide on airway inflammation and remodelling in a mouse model of asthma. Clin. Exp. Allergy 40:1266–1275.
Opina M.T.D. and Moore W.C. 2017. Phenotype-driven therapeutics in severe asthma. Curr. Allergy Asthma Rep. 17:10.
Ortega H.G., Yancey S.W., Mayer B., Gunsoy N.B., Keene O.N., Bleecker E.R., Brightling C.E., and Pavord I.D. 2016. Severe eosinophilic asthma treated with mepolizumab stratified by baseline eosinophil thresholds: A secondary analysis of the DREAM and MENSA studies. Lancet Respir. Med. 4:549–556.
Pavord I.D., Afzalnia S., Menzies-Gow A., and Heaney L.G. 2017. The current and future role of biomarkers in type 2 cytokine-mediated asthma management. Clin. Exp. Allergy 47:148–160.
Peters S.P., Kunselman S.J., Icitovic N., Moore W.C., Pascual R., Ameredes B.T., Boushey H.A., Calhoun W.J., Castro M., Cherniack R.M., Craig T., Denlinger L., Engle L.L., DiMango E.A., Fahy J.V., Israel E., Jarjour N., Kazani S.D., Kraft M., Lazarus S.C., Lemanske R.F., Lugogo N., Martin R.J., Meyers D.A., Ramsdell J., Sorkness C.A., Sutherland E.R., Szefler S.J., Wasserman S.I., Walter M.J., Wechsler M.E., Chinchilli V.M., and Bleecker E.R. 2010. Tiotropium bromide step-up therapy for adults with uncontrolled asthma. N. Engl. J. Med. 363:1715–1726.
Petsky H.L., Kew K.M., Turner C., and Chang A.B. 2016a. Exhaled nitric oxide levels to guide treatment for adults with asthma. Cochrane Database Syst Rev. 11: CD011440.
Petsky H.L., Kew K.M., Turner C., Kynaston J.A., and Chang A.B. 2016b. Exhaled nitric oxide (FeNO) levels to guide treatment for children with asthma: A cochrane systematic review. Eur. Respir. J. 48:PA4373.
Petsky H.L., Li A., and Chang A.B. 2017. Tailored interventions based on sputum eosinophils versus clinical symptoms for asthma in children and adults. Cochrane Database Syst. Rev. 2017. 8: CD005603.
Price D.B., Rigazio A., Campbell J.D., Bleecker E.R., Corrigan C.J., Thomas M., Wenzel S.E., Wilson A.M., Small M.B., Gopalan G., Ashton V.L., Burden A., Hillyer E.V., Kerkhof M., and Pavord I.D. 2015. Blood eosinophil count and prospective annual asthma disease burden: A UK cohort study. Lancet Respir. Med. 3:849–858.
Rabe K.F., Nair P., Brusselle G., Maspero J.F., Castro M., Sher L., Zhu H., Hamilton J.D., Swanson B.N., Khan A., Chao J., Staudinger H., Pirozzi G., Antoni C., Amin N., Ruddy M., Akinlade B., Graham N.M.H., Stahl N., Yancopoulos G.D., and Teper A. 2018. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N. Engl. J. Med. 378:2475–2485.
Ribeiro C.M.P., Hurd H., Wu Y., Martino M.E.B., Jones L., Brighton B., Boucher R.C., and O’Neal W.K. 2009. Azithromycin treatment alters gene expression in inflammatory, lipid metabolism, and cell cycle pathways in well-differentiated human airway epithelia. PLoS ONE. 4: e5806.
Schleich F., Brusselle G., Louis R., Vandenplas O., Michils A., Pilette C., Peche R., Manise M., and Joos G. 2014. Heterogeneity of phenotypes in severe asthmatics. The Belgian Severe Asthma Registry (BSAR). Respir. Med. 108:1723–1732.
Shaw D.E., Sousa A.R., Fowler S.J., Fleming L.J., Roberts G., Corfield J., Pandis I., Bansal A.T., Bel E.H., Auffray C., Compton C.H., Bisgaard H., Bucchioni E., Caruso M., Chanez P., Dahlén B., Dahlen S.E., Dyson K., Frey U., Geiser T., De Verdier M.G., Gibeon D., Guo Y.K., Hashimoto S., Hedlin G., Jeyasingham E., Hekking P.P.W., Higenbottam T., Horváth I., Knox A.J., Krug N., Erpenbeck V.J., Larsson L.X., Lazarinis N., Matthews J.G., Middelveld R., Montuschi P., Musial J., Myles D., Pahus L., Sandström T., Seibold W., Singer F., Strandberg K., Vestbo J., Vissing N., Von Garnier C., Adcock I.M., Wagers S., Rowe A., Howarth P., Wagener A.H., Djukanovic R., Sterk P.J., and Chung K.F. 2015. Clinical and inflammatory characteristics of the European U-BIOPRED adult severe asthma cohort. Eur. Respir. J. 46:1308–1321.
Sonnenberg G.F. and Hepworth M.R. 2019. Functional interactions between innate lymphoid cells and adaptive immunity. Nat. Rev. Immunol. 19:599–613.
Spagnolo P., Fabbri L.M., and Bush A. 2013. Long-term macrolide treatment for chronic respiratory disease. Eur. Respir. J. 42:239–251.
Szefler S.J., Murphy K., Harper T., Boner A., Laki I., Engel M., El Azzi G., Moroni-Zentgraf P., Finnigan H., and Hamelmann E. 2017. A phase III randomized controlled trial of tiotropium add-on therapy in children with severe symptomatic asthma. J. Allergy Clin. Immunol. 140:1277–1287.
Szefler S.J., Vogelberg C., Bernstein J.A., Goldstein S., Mansfield L., Zaremba-Pechmann L., Engel M., and Hamelmann E. 2019. Tiotropium is efficacious in 6- to 17-year-olds with asthma, independent of T2 phenotype. J. Allergy Clin. Immunol. Pract. 7:2286–2295.e4.
Tadrous M., Khuu W., Lebovic G., Stanbrook M.B., Martins D., Paterson J.M., Mamdani M.M., Juurlink D.N., and Gomes T. 2018. Real-world health care utilization and effectiveness of omalizumab for the treatment of severe asthma. Ann. Allergy, Asthma Immunol. 120:59–65.e2.
Tajiri T., Matsumoto H., Gon Y., Ito R., Hashimoto S., Izuhara K., Suzukawa M., Ohta K., Ono J., Ohta S., Ito I., Oguma T., Inoue H., Iwata T., Kanemitsu Y., Nagasaki T., Niimi A., and Mishima M. 2016. Utility of serum periostin and free IgE levels in evaluating responsiveness to omalizumab in patients with severe asthma. Allergy Eur. J. Allergy Clin. Immunol. 71:1472–1479.
Takayama G., Arima K., Kanaji T., Toda S., Tanaka H., Shoji S., McKenzie A.N.J., Nagai H., Hotokebuchi T., and Izuhara K. 2006. Periostin: A novel component of subepithelial fibrosis of bronchial asthma downstream of IL-4 and IL-13 signals. J. Allergy Clin. Immunol. 118:98–104.
Tan L.D., Yoneda K.Y., Louie S., Hogarth D.K., and Castro M. 2019. Bronchial thermoplasty: A decade of experience: State of the art. J. Allergy Clin. Immunol. Pract. 7:71–80.
Taylor D.R. 2006. Nitric oxide as a clinical guide for asthma management. J. Allergy Clin. Immunol. 117:259–262.
Taylor S.L., Leong L.E.X., Mobegi F.M., Choo J.M., Wesselingh S., Yang I.A., Upham J.W., Reynolds P.N., Hodge S., James A.L., Jenkins C., Peters M.J., Baraket M., Marks G.B., Gibson P.G., Rogers G.B., and Simpson J.L. 2019. Long-term azithromycin reduces haemophilus influenzae and increases antibiotic resistance in severe asthma. Am. J. Respir. Crit. Care Med. 200:309–317.
Tiotiu A. 2018. Biomarkers in asthma: state of the art. Asthma Res. Pract. 4:10.
Tyler S.R. and Bunyavanich S. 2019. Leveraging -omics for asthma endotyping. J. Allergy Clin. Immunol. 144:13–23.
Veen J.C.C.M., Smits H.H., Hiemstra P.S., Zwinderman A.E., Sterk P.J., and Bel E.H. 1999. Lung function and sputum characteristics of patients with severe asthma during an induced exacerbation by double-blind steroid withdrawal. Am. J. Respir. Crit. Care Med. 160:93–99.
Vonk J.M., Jongepier H., Panhuysen C.I.M., Schouten J.P., Bleecker E.R., and Postma D.S. 2003. Risk factors associated with the presence of irreversible airflow limitation and reduced transfer coefficient in patients with asthma after 26 years of follow up. Thorax. 58:322–327.
Wagener A.H., De Nijs S.B., Lutter R., Sousa A.R., Weersink E.J.M., Bel E.H., and Sterk P.J. 2015. External validation of blood eosinophils, FENO and serum periostin as surrogates for sputum eosinophils in asthma. Thorax. 70:115–120.
Wechsler M.E., Laviolette M., Rubin A.S., Fiterman J., Lapa e Silva J.R., Shah P.L., Fiss E., Olivenstein R., Thomson N.C., Niven R.M., Pavord I.D., Simoff M., Hales J.B., McEvoy C., Slebos D.-J., Holmes M., Phillips M.J., Erzurum S.C., Hanania N.A., Sumino K., Kraft M., Cox G., Sterman D.H., Hogarth K., Kline J.N., Mansur A.H., Louie B.E., Leeds W.M., Barbers R.G., Austin J.H.M., Shargill N.S., Quiring J., Armstrong B., and Castro M. 2013. Bronchial thermoplasty: Long-term safety and effectiveness in patients with severe persistent asthma. J. Allergy Clin. Immunol. 132:1295–1302.e3.
Wenzel S., Ford L., Pearlman D., Spector S., Sher L., Skobieranda F., Wang L., Kirkesseli S., Rocklin R., Bock B., Hamilton J., Ming J.E., Radin A., Stahl N., Yancopoulos G.D., Graham N., and Pirozzi G.2013. Dupilumab in persistent asthma with elevated eosinophil levels. N. Engl. J. Med. 368:2455–2466.
Winkler C., Hochdörfer T., Israelsson E., Hasselberg A., Cavallin A., Thörn K., Muthas D., Shojaee S., Lüer K., Müller M., Mjösberg J., Vaarala O., Hohlfeld J., and Pardali K. 2019. Activation of group 2 innate lymphoid cells after allergen challenge in asthmatic patients. J. Allergy Clin. Immunol. 144:61–69.e7.
Zazzali J.L., Raimundo K.P., Trzaskoma B., Rosén K.E., and Schatz M. 2015. Changes in asthma control, work productivity, and impairment with omalizumab: 5-year EXCELS study results. Allergy Asthma Proc. 36:283–292.
Zimmermann G.S., Neurohr C., Villena-Hermoza H., Hatz R., and Behr J. 2009. Anti-inflammatory effects of antibacterials on human bronchial epithelial cells. Respir. Res. 10:4–7.
Zissler U.M., Esser-Von Bieren J., Jakwerth C.A., Chaker A.M., and Schmidt-Weber C.B. 2016. Current and future biomarkers in allergic asthma. Allergy. 71:475–494.
Information & Authors
Information
Published In
LymphoSign Journal
Volume 6 • Number 4 • December 2019
Pages: 117 - 135
History
Received: 3 October 2019
Accepted: 16 October 2019
Accepted manuscript online: 4 November 2019
Copyright
© 2019.
Authors
Funding Information
None
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
Orit GourgyHacohen and ShaiCohen. 2019. Precision medicine applications for severe asthma. LymphoSign Journal.
6(4): 117-135. https://doi.org/10.14785/lymphosign-2019-0017
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item
View Options
View options
Login options
Check if you access through your login credentials or your institution to get full access on this article.
