Managing newborn screening for SCID in a referral centre
Abstract
Newborn screening for severe combined immunodeficiency was implemented in Ontario in August 2013. Infants identified by a positive newborn screen are referred in an orderly fashion for evaluation by an expert immunologist and, when appropriate, for immune function studies and treatment.
Statement of novelty: We demonstrate a novel flow chart for assessing and referring newborn screen-positive cases.
Severe combined immunodeficiency (SCID) is a potentially lethal disease unless treated early in life (Roifman 2017). Infants with SCID are susceptible to repeated and severe viral, bacterial and fungal infections. Nearly all patients die within the first 2 years of life if the hematopoietic system or gene defect is not repaired. The gold standard of treatment remains hematopoietic stem cell transplantation obtained from related or unrelated human leukocyte antigen (HLA) matched donors (Dalal et al. 2000; Grunebaum et al. 2006).
During T cell maturation, the T cell receptor gene undergoes recombination, creating a by-product of single strand DNA circles (T cell receptor excision circles; TRECs). Douek and colleagues (Douek et al. 1998) were the first to exploit this phenomenon as a marker for thymic production of mature T cells. TREC copy numbers are at the highest level during infancy.
Assessment of TREC levels as a universal screening method to detect SCID was established by Routes and colleagues in 2009 (Routes et al. 2009). Newborn screening (NBS) for SCID is performed using a quantitative real-time polymerase chain reaction (qRT-PCR) assay using dried blood spots collected as part of screening for other newborn conditions. This approach was found to be effective in detecting SCID and other types of severe T cell lymphopenia (Comeau et al. 2010; Kwan et al. 2014; Vogel et al. 2014). Yet, major limitations have been noted with the expansion of experience. Certain types of phenotypical SCID, such as Zap70 deficiency, can evade detection and most cases of non-SCID profound combined immunodeficiencies (CID) are not identified by this approach (Kobrynski 2015). Further, the test cannot discriminate between SCID and a variety of other conditions such as prematurity and maternal/infant exposure to certain medications.
Advocacy for implementing NBS for SCID in Canada was initiated and propelled by Roifman and Immunodeficiency Canada in 2013, through multiple presentations and a program submission to the Ministry of Health, Ontario. Chakraborty and colleagues from NBS Ontario (NSO) joined the effort and, upon approval, implemented the dried blood spot-based TREC tests. If screen-positive for SCID, samples are also tested in the NBS laboratory for adenosine deaminase (ADA) metabolites as well as 22q11. NBS-positive reports are sent to already established NBS Retrieval Centres operated by genetic counsellors to facilitate retrieval of the affected infant. A novel algorithm for assessing and referring NBS-positive cases is shown in Figure 1.
Figure 1:
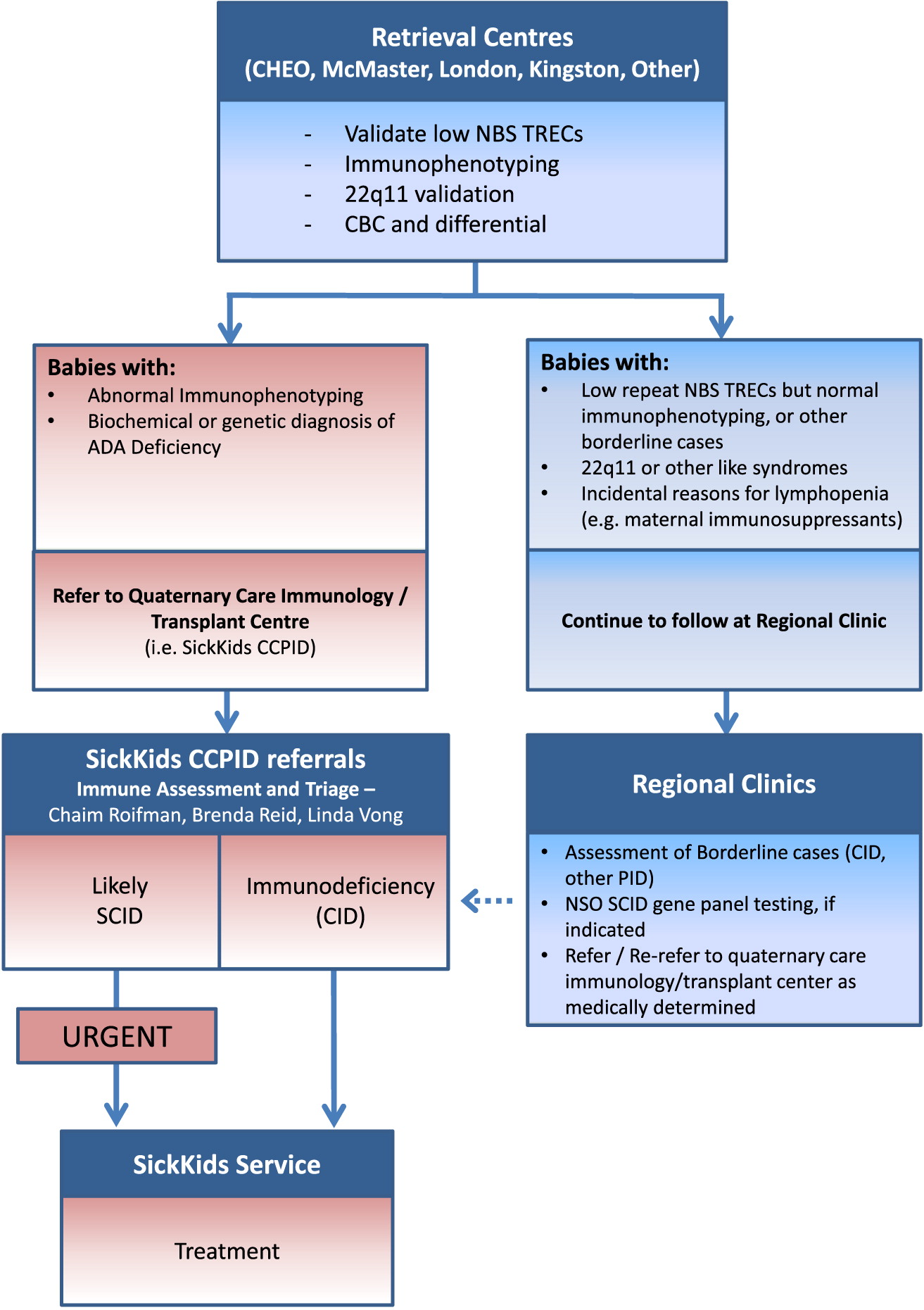
Retrieval Centres validate positive NBS by completing an initial family history screen that identifies any pre-existing conditions in the extended family and arranging for repeat blood work including repeat TREC testing, assessment of CBC and differential, immunophenotyping, and 22q11 microdeletion. Each Retrieval Centre has an identified physician associated with the SCID NBS program that is available to the genetic counsellor for consultation.
Babies with abnormal immunophenotyping or suspected cases of ADA deficiency are referred as soon as possible to a Quaternary facility for more extensive immune evaluation and assessment of therapeutic plans. The team consists of immunologists with expertise and experience in managing primary immunodeficiency, including SCID (Canadian Centre for Primary Immunodeficiency, CCPID; SickKids). Upon the diagnosis of SCID, the infant is urgently presented to the Immunology service team to develop a treatment plan.
If determined to be a non-SCID case with abnormal repeat NBS TRECs and various changes in immunophenotyping as well as atypical 22q11-like syndromes, the baby may be followed initially at regional clinics. Regional immunologists can request genetic SCID panel analysis and (or) refer borderline cases suspected of having CID to the Quaternary centre. If a firm diagnosis of profound T cell deficiency (CID) is made, the infant will be directed for formulation of appropriate treatment in this centre.
The development and implementation of this algorithm for NBS for SCID has provided a standardized approach across the province in the management of SCID infants. It facilitates early retrieval and confirmation of the diagnosis of SCID in babies prior to the development of any symptoms of the disease, and allows for the early implementation of a plan of care, which has been shown to improve overall outcomes for these patients.
REFERENCES
Comeau A.M., Hale J.E., Pai S.Y., Bonilla F.A., Notarangelo L.D., Pasternack M.S., Meissner H.C., Cooper E.R., DeMaria A., Sahai I., and Eaton R.B.2010. Guidelines for implementation of population-based newborn screening for severe combined immunodeficiency. J. Inherit. Metab. Dis.33:273–281.
Dalal I., Reid B., Doyle J., Freedman M., Calderwood S., Saunders F., and Roifman C.M.2000. Matched unrelated bone marrow transplantation for combined immunodeficiency. Bone Marrow Transplant.25:613–621.
Douek D.C., McFarland R.D., Keiser P.H., Gage E.A., Massey J.M., Haynes B.F., Polis M.A., Haase A.T., Feinberg M.B., Sullivan J.L., Jamieson B.D., Zack J.A., Picker L.J., and Koup R.A.1998. Changes in thymic function with age and during the treatment of HIV infection. Nature. 396:690–695.
Grunebaum E., Mazzolari E., Porta F., Dallera D., Atkinson A., Reid B., Notarangelo L.D., and Roifman C.M.2006. Bone marrow transplantation for severe combined immune deficiency. JAMA. 295:508–518.
Kobrynski L.2015. Newborn screening for severe combined immune deficiency (technical and political aspects). Curr. Opin. Allergy Clin. Immunol.15:539–546.
Kwan A., Abraham R.S., Currier R., Brower A., Andruszewski K., Abbott J.K., Baker M., Ballow M., Bartoshesky L.E., Bonilla F.A., Brokopp C., Brooks E., Caggana M., Celestin J., Church J.A., Comeau A.M., Connelly J.A., Cowan M.J., Cunningham-Rundles C., Dasu T., Dave N., De La Morena M.T., Duffner U., Fong C.T., Forbes L., Freedenberg D., Gelfand E.W., Hale J.E., Hanson I.C., Hay B.N., Hu D., Infante A., Johnson D., Kapoor N., Kay D.M., Kohn D.B., Lee R., Lehman H., Lin Z., Lorey F., Abdel-Mageed A., Manning A., Mcghee S., Moore T.B., Naides S.J., Notarangelo L.D., Orange J.S., Pai S.Y., Porteus M., Rodriguez R., Romberg N., Routes J., Ruehle M., Rubenstein A., Saavedra-Matiz C.A., Scott G., Scott P.M., Secord E., Seroogy C., Shearer W.T., Siegel S., Silvers S.K., Stiehm E.R., Sugerman R.W., Sullivan J.L., Tanksley S., Tierce M.L.T., Verbsky J., Vogel B., Walker R., Walkovich K., Walter J.E., Wasserman R.L., Watson M.S., Weinberg G.A., Weiner L.B., Wood H., Yates A.B., Puck J.M., and Bonagura V.R.2014. Newborn screening for severe combined immunodeficiency in 11 screening programs in the United States. JAMA. 312:729–738.
Roifman C.M.2017. Primary T-cell immunodeficiencies. In Rich R.R., ed. Clinical immunology principles and practice. 5th ed. Elsevier.
Routes J.M., Grossman W.J., Verbsky J., Laessig R.H., Hoffman G.L., Brokopp C.D., and Baker M.W.2009. Statewide newborn screening for severe T-cell lymphopenia. JAMA. 302:2465–2470.
Vogel B.H., Bonagura V., Weinberg G.A., Ballow M., Isabelle J., Diantonio L., Parker A., Young A., Cunningham-Rundles C., Fong C.T., Celestin J., Lehman H., Rubinstein A., Siegel S., Weiner L., Saavedra-Matiz C., Kay D.M., and Caggana M.2014. Newborn screening for SCID in New York State: Experience from the first two years. J. Clin. Immunol.34:289–303.
Information & Authors
Information
Published In

LymphoSign Journal
Volume 4 • Number 2 • June 2017
Pages: 77 - 79
History
Received: 11 April 2017
Accepted: 18 May 2017
Accepted manuscript online: 29 May 2017
Copyright
© 2017.
Authors
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
BrendaReid, AdiOvadia, and Yael DinurSchejter. 2017. Managing newborn screening for SCID in a referral centre. LymphoSign Journal.
4(2): 77-79. https://doi.org/10.14785/lymphosign-2017-0005
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
Cited by
1. Management of newborn screening for severe combined immunodeficiency at a quaternary referral centre—an updated algorithm
2. An unusual presentation of DiGeorge syndrome
3. Report of the Canadian Expert Committee on the management of ADA deficiency
4. Abstracts from the Immunodeficiency Canada—7th SCID Symposium, Montreal, QC, 24 October 2019
View Options
View options
Get Access
Login options
Check if you access through your login credentials or your institution to get full access on this article.
